
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted November 9, 2020: by Bill Sardi
If you believe people test COVID-19 positive and therefore are infected but have no symptoms, I have a bridge to sell you in New York very cheaply. Yes, I too fell for this modern fairy tale in the early days of the pandemic. After all, this “fact” was cited in the most prestigious medical journals. Modern medicine foists off this falsehood and we’re supposed to believe it, cancel sports, church, and family events, all over one symptomless person who tested positive for COVID-19 coronavirus. In fact, if COVID-19 infected patients aren’t experiencing even a mild fever, they aren’t developing antibodies against the disease.
And doctors say President Trump tested positive, was hospitalized for 3-days (it was a hotel room inside a hospital) and then showcased an antiviral drug (Remdesivir) for an American company (Trump should have been paid an endorsement fee); then Trump took off his mask and declared himself cured. But hey, Trump is no medicine man who knows science. He wouldn’t know any better. And neither would any of his narrow-minded doctors. In modern medicine, everything is treated as if it is a drug deficiency. Doctors are never going to cure COVID-19 as long as they have their nutritional deficiency blinders on.
But Mr. Trump did say: ““When you test, you create cases.” “If we stop testing right now, we’d have very few cases, if any.”
The disease mongers and his political opponents jumped on the President for making that statement. But Mr. Trump was not ill advised to say that. It is true, because COVID-19 coronavirus is not killing people, the lockdown and news-media induced anxiety is. Here’s how.
First scrutinize a flawed test, the PCR (polymerase chain reaction test) that is known to start pseudo-epidemics, and realize:
A “mysterious, puzzling phenomenon”
Now it is within this context of overreliance on PCR testing that journalists at the Wall Street Journal began to investigate what they call “mysterious” long-term effects of COVID-19, “puzzling phenomenon” even among non-hospitalized young people, who are dealing with lingering symptoms, namely:
The WSJ reporters quoted a University of Oxford expert to say: initially “the disease itself is not that bad” but symptoms persist for months. The Oxford expert said: “Monitoring post-acute COVID-19 patients is not yet an exact science.” Frankly, maybe not science at all.
Large percentages of hospital discharged COVID-19 patients report mental depression, obsessive-compulsive behavior, anxiety, insomnia, post-traumatic stress disorder.
WSJ reporters go on to say “anxiety caused by social isolation and uncertainty surround the pandemic may exacerbate symptoms, though that isn’t likely the primary cause.” They’re wrong.
Here is what is really happening:
The medical director for Mt. Sinai Health System’s Center for Post-COVID-10 Care says: “I haven’t really seen any other illness that affects so many different organ systems in as many different ways as COVID does.” That’s because modern medicine casts a blind eye at nutritional therapy.
What IS causing all the symptoms of COVID-19 is a shortage of a critical B vitamin. Basically, what we are seeing on a worldwide basis is beri beri – vitamin B1 deficiency. A disease historically caused by famine but now caused caused by “high calorie malnutrition.”
Modern-trained doctors wouldn’t know a case of beri beri if they saw one because it is caused by a shortage of an essential vitamin that is known as a great disease masquerader. Doctors aren’t looking for vitamin deficiencies.
And yes, a deficiency of this vitamin may result in shortness of breath (dyspnea), the hallmark respiratory symptom for COVID-19. This shortness of breath is not caused by viral infection but a loss of automatic nerve control where the patient must begin to consciously work to breathe rather than automatically breathe.
A vitamin B1deficiency may be misdiagnosed as a viral infection or pneumonia.
A B-vitamin shortage can induce a loss of appetite which circuitously reduces dietary intake of B vitamins, which can biochemically result in loss of smell (anosmia), another hallmark symptom of COVID-19. (It has previously been noted that a shortage of the trace mineral zinc also induces anosmia –loss of smell– which is often the first symptom of COVID-19 infection, and this lingers in the post-infection period.
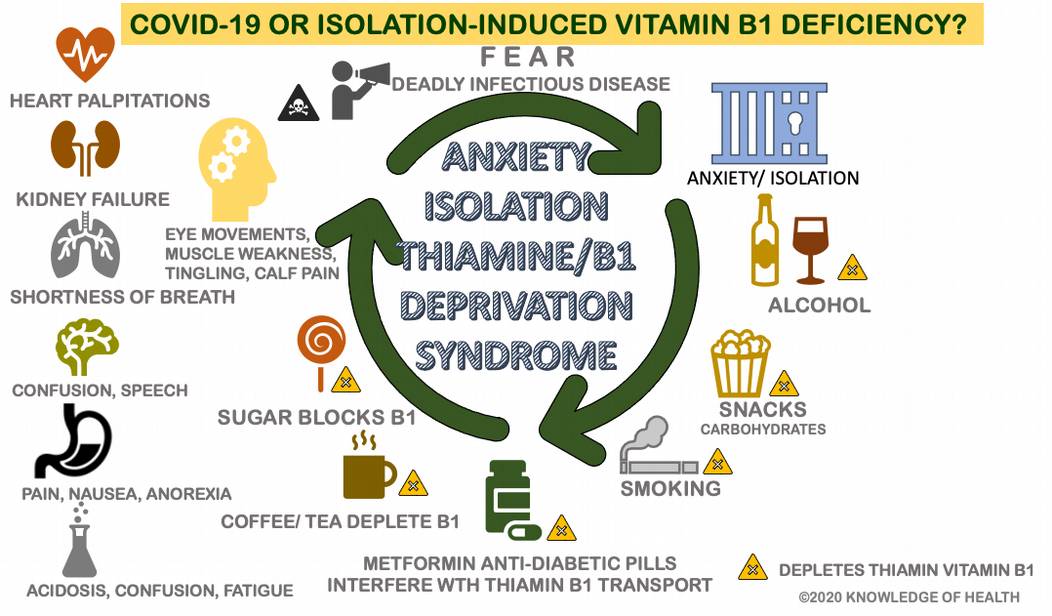
All of the above practices deplete this essential B vitamin, needed for our bodies to function automatically (heartbeat, digestion, respirations). The Wall Street Journal journalists quoted doctors to say “patients appear to be developing dysautonomia, dysregulation of the autonomic nervous system.”
This reporter’s investigation finds COVID-19 is not a viral infection but rather a B1-vitamin deficiency magnified by an anxiety-causing lockdown.
What a pandemic promoted societal lockdown does is similar to solitary confinement in its behavioral and mental aspects. Solitary confinement is “the worse kind of psychological torture,” that can cause irreversible psychological effects in as little as 15 days. Many Americans were already living alone, living lonely. Pandemic quarantines and required lockdown produce negative psychosocial outcomes, particularly among vulnerable individuals.
Fearful Americans may then overeat or have no appetite, drink too much alcohol, smoke more cigarettes, eat more sugary foods, lose more sleep and rely on stimulants like caffeine in coffee or tea, all which deplete vitamin B1.
One of the dilemmas facing physicians is that due to the lockdown, many people believed to be infected with COVID-19 coronavirus endured their symptoms at home and didn’t go to the hospital, fearful of being infected by doctors who are cross-infected from patients and other staff, and wary of the ventilator treatments that may be more harmful to the lungs than the disease.
Some patients experienced very mild symptoms at home such as loss of smell and taste. Thereafter, finally attending medical clinics, there were found to experience a 2nd round of symptoms that included muscle pain (myalgia), intense fatigue, sensation of fever, shortness of breath, racing heart (tachycardia), headaches, and anxiety.
Doctors were perplexed to find only a “small portion of these patients who sought aftercare had a proven history of COVID-19 as confirmed by PCR testing. Doctors concluded these symptoms were indicative of dysautonomia – loss of automatic control of the nervous system – – heartbeat, digestion and respirations. This concession was documented in a report published in the journal Clinical Microbiology & Infection, July 23, 2020. Dysautonomia is a vitamin B1 deficiency disease. Dare any doctor say this is a nutritional deficiency, not a viral epidemic?
Generally, COVID-19 coronavirus cases typically present as fever and respiratory illness, but almost 50% of cases also involve unexplained digestive symptoms that include nausea, vomiting, diarrhea and loss of appetite, all symptoms known to be caused by a vitamin B1 deficiency, not a stomach virus.
Sometimes digestive symptoms precede respiratory symptoms. There is general agreement among physicians that the virus infects the gastrointestinal tract. Laboratory reports claimed the virus was found to persist in stool samples. But the same flawed PCR test is used to make this mistaken claim.
Stress can lead to the onset and chronic overuse of alcohol.
Many thousands of Americans are closet alcoholics. That is why liquor stores were considered essential during the pandemic. There would have been hundreds of thousands of Americans going through alcohol withdrawal symptoms had they not had access to alcohol. According to a study, 1 in 8 American adults (12.7%) now meet the criteria for alcohol-use disorder. Alcoholic beverages deplete zinc, magnesium and vitamin B1.
This is a likely reason why COVID-19 death rates were so high in Italy. There are more than 14 million daily consumers of alcohol in Italy, many of them older men. Winos by another name. There is a dose-dependent correlation between viral infections and alcohol consumption. About 30-40% of alcoholics suffer from hepatitis C and HIV. The risk for pneumonia increases by 83% among heavy alcohol imbibers. But again, doctors mistakenly believe all these diseases are caused by microbial infection, not malnutrition.
Another continued claim is that COVID-19 is more prevalent among males than females. However, men are more likely to smoke and drink alcohol excessively than females.
An anecdotal report is telling. At a party in Thailand only those partygoers who drank a shared alcoholic beverage from the same glass were infected with COVID-19. Four partygoers who didn’t imbibe did not develop illness.
Consumption of mentally-numbing alcohol is a self-destructive way of coping with stress, damaging the brain and liver in particular. In the week ending 14th March 2020 the sales in the U.S. of beer, wine and alcoholic spirits increased by 14%, 28% and 26% respectively compared to the same period in the prior year. But numbers don’t tell all. Essentially alcohol disappeared from store shelves during March 2020. It was being hoarded. Because store shelves were empty, no more could be purchased.
The lockdown resulted in more sedentary Americans who spent more time in front of a TV set or computer screen, who either gained or lost weight, who smoked more and drank more alcohol. One survey reveals sleep disturbances were prevalent among 60.8% of adults during the COVID-19 lockdown. That results in more and more Americans drinking caffeinated beverages like coffee and tea. And here again, coffee and tea contain molecules that block the absorption of vitamin B1.
One study reveals that 36.4% of COVID-19 diagnosed patients have neurologic symptoms.
People who are vitamin B1-deficient (have beri beri) exhibit nervous system irregularities: numbness or tingling of the legs, arms, neck, inability to speak, difficulty swallowing, headaches from brain involvement. B1-deficients may can act like they are drunk (ataxia), lose weight due to loss of appetite or report vomiting and diarrhea.
COVID-9 is associated with meningitis, paralyzing Guillain-Barre syndrome, encephalitis (brain swelling), and various myopathies (degenerative muscle diseases), believed to be caused by the spread of the virus from the respiratory system (lungs) to the central nervous system. Inexplicably, not every COVID-19 patient with these nervous disorders tests positive for the virus in the cerebrospinal fluid. This is a tacit admission it isn’t COVID-19 that is causing this pandemic.
The time taken for the ventricles (pumping chambers of the heart) to contract and relax is called the QT interval. A prolonged QT interval is associated with heart failure and mortality. Drugs like hydroxychloroquine used to treat COVID-19 cases are reported to prolong the QT interval, though there is mixed science on this topic with such cases considered rare. A shortage of B1 has been cited to prolong the QT interval.
Eventually a shortage of vitamin B1 can result in congestive heart failure, what is called “wet beri beri,” where fluid fills around the heart.
The first stage of wet beri beri involves the dilation (widening) of peripheral blood vessels (arms, legs) which results in a decline in blood pressure, then the heart beats faster (tachycardia). The kidneys then detect a relative decline in fluid volume and respond by conserving salt which in turn results in fluid overload and swelling of extremities and eventually heart failure accompanied by restlessness, anxiety and visible bulging neck veins.
Then fluid can back up into the lungs, which is how the lungs become involved in this potentially mortal disease. Viral infection is not causing the heart to fail. The so-called cytokine storm that is attributed to lung congestion in infectious lung disease is over-estimated.
It is reported that infection may be a trigger of tachycardia (racing heart) with 28-41% of patients reporting onset after the 2002 SARS (severe acute respiratory syndrome). Even months after a so-called COVID-19 infection, doctors mistakenly believe the occurrence of a variety of symptoms are related to this viral infection.
The case of a patient who developed tachycardia (racing heart) of prolonged duration (5.5 months following initial COVID-19 symptoms) is an example. Autonomic testing revealed an exaggerated case of tachycardia upon climbing stairs (110 heart beats/minute when resting, 190 beats/minute after walking up a flight of stairs). But the patient’s doctors seem oblivious to the connection between dysautonomia and vitamin B1 deficiency.
Few published studies address thiamin B1 as a remedy for COVID-19 symptoms, particularly nervous system involvement. A conciliatory study points in a direction away from a coronavirus. It’s reported mega-dose thiamin (B1) supplementation reduces overresponsive T-helper cells among heavy drinkers, thus reducing the risk for a cytokine storm that can fill the lungs with fluid during COVID-19 infections. A prior report indicates a shortage of vitamin B1 may result in out-of-control T-cells. Researchers do concede it’s possible that patients with viral infection could have an increased risk for thiamin deficiency. But their interpretation is that viral infection depletes thiamin rather than thiamin deficiency induces over-active T-cells and lung inflammation.
Using a stethoscope, doctors frequently hear crackle sounds in the lungs of COVID-19 patients. Crackle sounds in the lungs are not specific for any particular infectious disease but they are widely associated with vitamin B1 deficiency. Here is the evidence:
What may be missed by acute care physicians is that fever with pneumonia among some patients may not be induced by a germ but may be induced by a vitamin B1 deficiency that results from loss of control of body temperature by the hypothalamus in the brain.
Few physicians recognize thiamine deficiency can result in high fever. Vitamin B1 injections may eradicate infections. A fever accompanied by vitamin B1 malnutrition may emanate from dysfunction of the hypothalamus in the brain with accompanying lack of nitric oxide, a transient gas in the blood circulation needed to quell infections.
In many cases of pneumonia no bacterial or viral infection is identified.
Vitamin B1 therapy should be a standard therapy for any patient with lung disease and a history of alcohol or tobacco consumption should call for vitamin B1 testing upon hospital admission.
At the start of the pandemic in January of 2020 many Americans were living on the edge of a beri beri epidemic regardless of COVID-19.
It only takes 18 days to develop a vitamin B1 deficiency. A typical diet provides no more than 1-2 milligrams of this water-soluble vitamin that needs daily replacement.
Nicotine and alcohol use deplete essential nutrients like vitamin B1 and vitamin C. In China, where the COVID-19 epidemic is said to have started, 68% of men are smokers and 46% drink alcohol.
According to Derrick Lonsdale MD and Chandler Marrs PhD, the following percentages of Americans are living on the edge of mortal consequences because of their shortage of thiamin (vitamin B1) that is being misdiagnosed as a viral infection:
76% of diabetics (adult and child onset)
29% of obese patients; 49% of bariatric patients
40% of community dwelling elderly; 48% in acute care
55% of cancer patients
20% of ER patients
33% of congestive heart failure patients
38% of pregnant women (more with nausea and vomiting)
30% of psychiatric patients
Modern medicine is so compartmentalized that it is difficult to conceive a disease like beri beri is so anatomically and physiologically permeating. Beri beri is so pervasive it defies conventional diagnosis. This author must expand the broad signs and symptoms caused by vitamin B1 deficiency, as the Mayo Clinic has done with its expanded list of symptoms below.
THIAMINE (thiamin) vitamin B1Molecular formula: C12H17N4OS+ Molecular weight: 265.36 grams/mol
Thiamine (aka thiamin) is a colorless compound that is a water-soluble essential vitamin, belonging to the B-vitamin family, with mood modulating, sugar-regulating activities. Thiamine is necessary for metabolism of carbohydrate, protein and fats. Thiamine is required for the production of adeno-triphosphate (ATP), the cell’s energy currency.
Thiamine was first discovered by Umetaro Suzuki in Japan when researching how rice bran cured patients of Beriberi.
Thiamine cannot be stored in the body; about 80% of thiamine is in red blood cells; however, once absorbed it is concentrated in muscle tissue.
In a state of true deficiency, it may induce its most visible symptom, horizontal eye movements (nystagmus), often mistaken for illicit drug use. In the elderly a B1 deficiency may result in premature senility and confabulations – making up stories to fill in gaps in memory.
In a misdirection, one study shows 25% of British millennials mistakenly believe a vegan diet is more appealing since the worldwide outbreak of COVID-19. Yet a vegan diet may not resolve a B1 deficiency. Not unless coffee/tea, alcohol, tobacco, anti-diabetic medicines (metformin), diuretics and sugary foods are abandoned.
In a dietary survey conducted in a European country, 52% reported snacking more during the lockdown.
Beef, liver, eggs, fish, pork are major dietary sources of B1 along with seeds (flaxseed), nuts and beans. But with so many B1 blockers in use (carbohydrates, sugar, alcohol, coffee/tea), even a B1 fortified diet may not be enough to quell a vitamin deficiency epidemic.
It is not a coincidence that a list of anti-depressant foods supply vitamin B1 along with zinc, vitamin A, C, D.
In our modern world with a plethora of prepared and processed convenience foods, the best way to ensure adequate B1 nutrition is to supplement the diet with B1 pills. A fat-soluble form of B1 benfotiamine (ben-fo-tee-ah-meen) is recommended. Allithiamine is another fat-soluble form of B1 that passes through the blood/brain barrier. There is no overdose for B1 supplementation.
In the face of so many factors that impair B1 absorption (alcohol, coffee, tea, sugar, carbohydrates, medicines), B1 supplementation would be required to quell a B1 pandemic. It’s probably best to supplement with vitamin B1 at a different time than when coffee or tea is consumed.
Don’t trust your diet to prevent or cure. Thiamine is a water-soluble vitamin that is easily washed out of the body. Those individuals who take water pills (diuretics) unwittingly develop shortage of B1 and suffer with symptoms that are not readily connected with B1 deficiency. Individuals who take antacids and contraceptive pills are also at increased risk for B1 deficiency. Older adults secrete less stomach acid and absorb less and less thiamin from their diet as they age. An acid supplement (betaine) improves B1 absorption.
The World Health Organization (WHO) should know better. It fails to heed its own body of knowledge, namely a report entitled: “Thiamine Deficiency And Its Prevention And Control In Major Emergencies.” Historical epidemics of thiamin deficiency are well documented by the WHO. But the WHO generally presents beri beri as a consequence of food deprivation in third-world countries, not a rampant epidemic in advanced countries due to “high calorie malnutrition” as explained by Derrick Lonsdale MD.
The great masquerader, beri beri, has fooled the world once again. It is misdiagnosed as this disease or that disease. In modern medicine a B1-deficiency is seen by cardiologists, neurologists, pulmonologists, psychiatrists, virologists, bacteriologists, ophthalmologists, nephrologists, hepatologists, who are simply not trained that beri beri cannot be anatomically compartmentalized like other diseases.
Because modern medicine is looking in all the wrong places to cure and prevent COVID-19, there will never be a cure. The world will be held in perpetual lockdown. Vaccination will be an exercise in frustration. The cure will be more deadly than the disease.
It is worth mentioning that The World Economic Forum (WEF) out of Europe says it is time for global government to exert world leadership in a crisis such as the COVID-19 epidemic. The WEF is part of a global conspiracy to force vaccination, abandon paper money, and drastically reduce meat consumption to a point where it is only consumed as an occasional delicacy, a practice which would further exacerbate the ongoing vitamin B1 deficiency epidemic now in progress. Ironically, the worldwide lockdown is causing workers to not show up for work for fear of infection. This is beginning to cause food shortages that could lead to famines and the return of beri beri epidemics of the past.
Posted in Coronavirus ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105