
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted April 14, 2017: by Bill Sardi
Key points:
If your cardiologist didn’t prescribe zinc during your last office, he/she should have.
It turns out there is more evidence that maintenance of zinc levels reduce mortality rates for coronary heart disease than there is proof that statin cholesterol-lowering drugs save lives.
Half of all patients with coronary heart disease do not have any of the established coronary risk factors. [American Journal Critical Care 1998] Control of circulating cholesterol by limiting its production in the liver with statin drugs is the main focus of modern medicine in an effort to prevent the leading cause of death in America – coronary artery heart disease. But in reality, three of every four heart attacks are of the sudden-death variety and are caused by an electrical storm in the heart, not by cholesterol-induced blockage of coronary arteries. [Circulation 2001]
Supplemental minerals would likely save more lives than an array of today’s cardiac drugs like calcium blockers and beta blockers. To prevent these types of electrical conduction heart attacks the provision of cardiac electrolytes such as magnesium and potassium would be more appropriate than cholesterol-lowering drugs. [Hippokratia Oct-Dec 2006; Experimental Clinical Cardiology Winter 2010]
Efforts to halt or reverse atherosclerosis, defined as hardening and narrowing of the arteries, ignore the fact zinc and copper play a primary underlying role in maintenance of arterial health.
Statin drugs, introduced in 1987 (Mevacor), artificially lower circulating levels of total and LDL (low-density lipoproteins) by 20-63% and are reported to increase HDL (high-density lipoproteins) by 5-15%. HDL cholesterol is called reverse cholesterol because it transports cholesterol out of artery walls and back to the liver for disposal.
But even the alleged advantage of maintaining high HDL cholesterol levels is now being questioned. High-dose niacin, which raises HDL cholesterol, was found to be ineffective. Cardiologists are backing away from the idea of raising HDL levels. [Cleveland Clinic April 8, 2016]
While statin drugs do reduce circulating cholesterol levels by slowing their synthesis in the liver where 80% of cholesterol is produced (only 20% of cholesterol comes from the diet), statins only reduce the risk for non-mortal heart attacks by 1 in 200 healthy adults and 1 in 70 high-risk adults over a 5-year period. [Bloomberg News Jan 16, 2008]
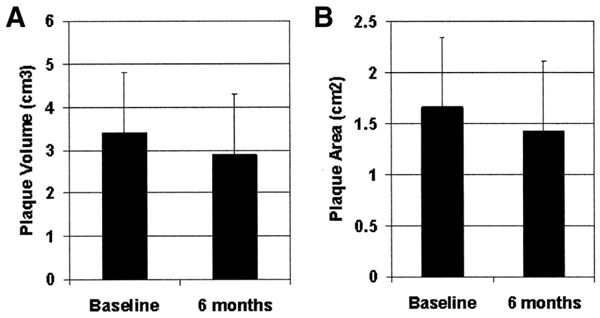
The reduction of arterial plaque accomplished by statin drugs is slow. Over years of time plaque volume is reduced. But the patient at high risk for a heart attack is falsely led to believe a statin drug will immediately save their life.
After six months plaque volume and plaque area are only modestly reduced (see graphs below). Only 1% of the plaque is reduced over a 6-month period of time. [Circulation Oct 19, 2004] In another study, plaque volume was only reduced by 11.1% over a 10-month treatment period with a statin drug. [Circulation Journal June 2016]
Furthermore, statistically significant reduction in plaque burden is only achieved with high-dose statin therapy, which increases the risk for drug side effects. Moreover, the reduction in fibrous plaque volume is offset by an increase in calcium deposition. [BMC Medicine 2015]
Frankly there is more convincing evidence that a shortage of zinc raises cardiac mortality rates while cholesterol reduction has a null effect in preventing cardiac death, though statin cholesterol-lowering drugs do prevent non-mortal heart attacks.
American adults consume less than 10 milligrams of zinc per day but only absorb maybe ~2-3 milligrams. The Recommended Daily Allowance for zinc is 11 mg/day for males and 8 mg/day for females. The safe upper limit for zinc intake is 40 mg/day. [Office Dietary Supplements]
A population study that delved into the association between zinc, copper and magnesium in regard to mortality is telling. The highest blood levels of copper were associated with a 50% increase in mortality from all causes and a 30% increase for cardiovascular deaths. High blood serum magnesium was protective and reduced mortal risk by 40% for all causes and cardiovascular deaths. A combination of low zinc and high copper increased the risk for all-cause death by 260%. [Epidemiology May 2006]
While mortality studies involving zinc are sparse, one study of 346 subjects 80 year or older found a high copper over zinc ratio increased the risk for death by 1.9 fold. [Age June 2012] Another study involving 230 men dying from cardiovascular diseases reported high blood serum copper levels and low serum zinc concentrations were significantly associated with increased mortality from coronary artery disease in particular. The highest/lowest relative risk for cardiovascular disease mortality ranged from 2.86 to 0.69 between lowest and highest blood serum levels of copper and zinc. [European Journal Clinical Nutrition 1996]
Compare the above numbers with the relative mortality risk attributed reduction of circulating cholesterol with statin drugs, which ranges from 0.98 to 1.15 (up to 1.00 = no elevated risk). Translation: statin drugs have a null effect on mortality. In a landmark report, investigators conclude that cholesterol is an overestimated risk factor and “public health recommendations regarding the ‘dangers’ of cholesterol should be revised.” Among women, elevated cholesterol actually appears to be protective. [Journal Evaluation Clinical Practice Feb 2012]
By ignoring the importance of zinc and treating atherosclerosis as if it is a statin drug deficiency, it appears modern cardiology has been side tracked for the past 40+ years.
Furthermore, while zinc potentially reduces coronary artery calcification, statin drugs promote coronary calcification. [Medscape.com April 2, 2015; Journal American College Cardiology April 2015]
Like many drugs, statins circuitously induce the very disease they are intended to treat. Here is the evidence:
If you think of taking a zinc pill along with your statin drug, it might not be the best idea. Copper and zinc impair the ability of statin drugs to reduce synthesis of cholesterol from the liver. [Molecular Biosystems Feb 2011]
Over two decades ago it was shown that low zinc intake levels are associated with elevated blood plasma levels of cholesterol and LDL cholesterol. [Journal Nutrition Elderly 1993]
In 1994 it was noted that zinc prevents oxidation of LDL cholesterol and “consequently stops the main mechanism of atherosclerosis.” [Minerva Medicine Dec 1994]
Over 40 years ago a paper published in the American Journal of Clinical Nutrition said this:
Epidemiologic and metabolic data are consonant with the hypothesis that a metabolic imbalance in regard to zinc and copper is a major factor in the etiology of coronary heart disease. This metabolic imbalance is either a relative or an absolute deficiency of copper characterized by a high ratio of zinc to copper. The imbalance results in hypercholesterolemia and increased mortality die to coronary heart disease. The imbalance can occur due to the amounts of zinc and copper in human food, to lack of protective substances in food or drinking water and to alterations in physiological status that produce adverse changes in the distribution of zinc and copper in certain important organs. Because no other agent, with the possible exception of cholesterol, has been related so closely to risk, the ratio of zinc to copper may be the preponderant factor in the etiology of coronary heart disease. [American Journal Clinical Nutrition July 1975]
That was 12 years prior to the introduction of the first cholesterol-lowering statin drug (Mevacor in 1987).
But by 1980 researchers concluded otherwise. They said: “dietary copper and zinc levels, at levels likely to occur in a normal mixed diet, are not significant factors in cholesterol metabolism.” [American Journal Clinical Nutrition May 1980]
Six years later other researchers repeated the same finding, that “there is no association between plasma zinc or copper and the serum levels of lipids or lipoproteins; we believe that this indicates that these trace metals are of doubtful value as markers for coronary atherosclerosis.” [Atherosclerosis Nov 1986]
A polarized view of what causes atherosclerotic arterial disease emerged.
By the summer of 2003 researchers wanted to put the argument to bed. They tested the upper safe limit of zinc, 40 milligrams per day in male adults. Study participants were given a 30 milligram zinc tablet + 10 milligrams of estimated zinc from the diet for 14 weeks followed by the addition of 3 milligrams a day of copper for 8 more weeks. These subjects were compared against a group that took an inactive placebo pill. No effect of zinc supplementation was found on copper status or cholesterol metabolism. [Biology Trace Element Research Summer 2003] Hopes of employing zinc therapy for atherosclerosis were dashed.
In 2002 researchers analyzed data among elderly patients given high-dose zinc (80 mg zinc oxide/day) for treatment of an eye disease – macular degeneration. After 5 years there were no significant differences in copper or cholesterol levels between groups that received copper and zinc or copper or zinc singularly. Dietary zinc intake was similar to the general population. [Journal Nutrition April 2002] But long-term analysis reveals this mega-dose zinc therapy for the eyes did reduce mortality risk by 27%! [Archives Ophthalmology May 2004]
These conflicting reports concerning zinc and coronary artery disease may be explained by a research study, which showed that blood serum zinc levels were not associated with the prevalence or severity of coronary artery disease, but slower urinary loss of zinc was found to correlate with reduced risk for coronary artery disease as well as the prevalence of diabetes. A low blood serum zinc/urine zinc ratio is associated with severity of atherosclerosis. [Angiology July 2010]
Certainly diuretics (water pills) come to mind as obvious agents that deplete zinc via urinary excretion and therefore would nullify zinc’s anti-atherosclerotic properties. [Journal Hypertension (supplement) Dec 1984; South African Medical Journal Dec 1983]
There has been a marked increase in the use of diuretics as first-line therapy for high blood pressure. [Journal American Medical Assn. Nov 3, 2015] In 2003, 19.1% of 217.6 million American adults age 18 and older received treatment for high blood pressure and 46.3% used a diuretic. [Statistical Brief #119, Agency Health Care Policy Research, March 2008]
ACE inhibitors, commonly used to control blood pressure, also deplete zinc. [Metabolism July 1990; Journal American College Nutrition Feb 1998]
Zinc, by virtue of its ability to inhibit LDL oxidation, is an endogenous protective factor against atherosclerosis. [FEBS Letters March 21, 1994]
The oxidation of LDL particles describes the initial step of atherosclerosis, which damages the internal lining (endothelium) of the arteries. This initial injury triggers inflammation and an immune response with arrival of white blood cells (monocytes and T-lymphocytes) that increase blood-clotting tendencies.
White blood cells called monocytes that adhere to the surface of the endothelium are transported into the arterial wall and convert to another type of white blood cell called macrophages that release inflammatory factors within the vessel walls.
High circulating levels of LDL and low levels of HDL are independent predictors of atherosclerosis. For each 30 mg/deciliter decrease in LDL(c) confers with ~30% relative decrease in coronary artery disease risk.
Atherosclerotic plaque within cholesterol-fed rabbit arteries contains high levels of iron and reduced levels of zinc. Zinc supplementation reduces plaque area via displacement of iron and accumulation of calcium. Calcium plaque is less likely to rupture and block circulation in a coronary artery. [Arteriosclerosis Thrombosis Vascular Biology 2008]
More recently it has been realized that instead of statin drugs rupture of plaque and blockage of coronary artery blood circulation, statin drugs lead to plaque healing and stability. Instead of plaque regression there is plaque “healing,” though it is incomplete healing. [BMC Medicine 2015]
In a study of surgically removed carotid (neck) arteries, blood serum copper levels were higher in patients with hemorrhagic plaque in comparison to calcified plaque. Zinc concentrations were statistically lower in plaques of patients with fatty-fibrous plaque versus calcified plaque. The conclusion drawn from this study was that high circulating copper and lower circulating zinc levels may contribute to atherosclerosis. [Military-Medical and Pharmaceutical Review Sept 2015]
Ananda S Prasad of Wayne State University School of Medicine is the most noted authority on zinc and health in the world. Dr. Prasad’s studies show that zinc deficiency increases the generation of inflammation and induces dysfunction in the inner lining (endothelium) of arteries. Dr. Prasad found 30-40% of healthy elderly subjects in one US metropolitan area were zinc deficient. Zinc deficiency correlated with molecules sticking to the endothelial arterial linings and greater oxidation of fats (lipid peroxidation). Dr. Prasad reports mega-dose zinc supplementation effectively lowers blood plasma C-reactive protein (CRP) levels. [Advances Nutrition 2013]
Indeed, statin drug therapy reduces C-reactive protein levels, a marker of inflammation. [Atherosclerosis April 2016]
Zinc supplementation has been found to reduce C-reactive protein, a marker of inflammation that cardiologists often use independent of other risk factors such as cholesterol, age and smoking.
While caution is advised when consuming high-dose zinc because of an imbalance in the zinc/copper ratio, 45 milligrams of zinc/day was not found to decrease the copper status of elderly individuals. [American Journal Clinical Nutrition June 2010]
Meta-analysis is a statistical review of combined data obtained from multiple studies. A meta-analysis shows zinc supplementation had no effect upon blood cholesterol levels. [Atherosclerosis 2010] But lumping all zinc studies where varying doses of zinc were employed may confuse the issue. Of the 20 studies in one meta-analysis, 7 employed 100 mg of zinc or more which may induce strong binding of zinc to its binding protein (metallothionein) rendering it non-bioavailable. Fourteen (14) of the twenty studies utilized 50 mg or more of zinc. Different types of zinc were also employed. [Atherosclerosis 2010] This type of meta-analysis just leads to confusion.
Whatever concerns there are over zinc/copper ratios and cholesterol, they don’t apply to children. [Journal American College Nutrition 1989; Science Total Environment 1985] The fact children are not accumulating iron in their growing years because most of their dietary intake of iron is being used to make red blood cells may explain why cholesterol is not a problem for children.
Despite the promise of zinc therapy, more failed zinc studies are not difficult to find.
The provision of 50 mg or 75 mg zinc tablets to males had no effect upon serum levels of total cholesterol or LDL cholesterol. However, HDL cholesterol levels were significantly reduced. [American Journal Clinical Nutrition June 1988]
Similarly, in 2006 researchers concluded that controlled trials showed that total cholesterol and LDL blood concentrations were unaffected by supplementation with up to 150 mg of zinc per day. They also reported that when zinc supplements over 50 mg/day were used, blood plasma HDL cholesterol levels declined. [Journal American College Nutrition Aug 2006] Their analysis left researchers confused and no conclusion could be drawn.
In another study the provision of 150 mg/day of zinc to healthy young adults resulted in a decline in LDL cholesterol in females only. [Atherosclerosis April 1988]
In 1987 researchers wondered if elevated zinc over copper ratio is a risk factor for cardiovascular disease via alteration of cholesterol. They found that when serum copper levels were elevated and the serum zinc concentration was decreased, circulating levels of cholesterol rose. [Pathology Biology April 1987]
A more recent study analyzed mineral content in atherosclerotic plaque of surgically removed carotid arteries. Tissue copper levels were higher in patients with hemorrhagic versus calcified plaque. The conclusion drawn from this study was that high copper and lower zinc tissue levels were associated with atherosclerosis. [Military-Medical and Pharmaceutical Review Sept 2015]
Analyzing zinc intake levels or zinc blood levels without determination of copper status may be one obvious reason for the scientific confusion. There are other confounding factors.
Another reason why supplemental zinc may not be effective is competition for absorption from other minerals. Furthermore, the widespread use of iron and calcium supplements that are popular nowadays, both which interfere with zinc absorption and zinc activated enzymes, may exacerbate atherosclerosis via blockage of zinc. [Food & Function May 18, 2016]
The adult human body contains about 2000-3000 milligrams of zinc. In a state of perfect health all minerals in the body bound to a protein. Copper is bound to ceruloplasmin. Iron is bound to ferritin, albumin, transferrin (during transport), lactoferrin (during infection), and melanin (in skin, eyes, brain). Zinc is bound to metallothionein (me·tal·lo·thi·o·ne·in).
Zinc is the major mineral that binds to metallothionein. Zinc itself could potentially induce heart damage except for its controller metallothionein. [Circulation 2006]
Some free unbound zinc is important in reducing adhesion of molecules of white blood cells to the inner lining (endothelium) of blood vessels. [Cell Physiology 2010]
The antioxidant function of metallothionein was first proposed in the 1980s. [Experimental Biology & Medicine Dec 1999]
Metallothionein controls the amount of zinc available to tissues. Metallothionein binds to both copper and zinc but is reported to have a much greater affinity for copper. However excessive metallothionein can impair availability of both copper and zinc to tissues. Zinc deficiency induces a deficiency of metallothionein. [International Journal Clinical Experimental Medicine 2015]
It is endogenously produced metallothionein that protects the heart from toxic drugs cancer-treatment drugs like doxorubicin. [Journal Clinical Investigation 1997] This suggests supplemental zinc should be given concurrently with toxic cancer drugs.
The lack of metallothionein is associated with alcohol-induced scarring of the heart. Excessive alcohol given to rodents under experimental conditions produces fibrosis (scarring) of the heart. When mice were bred to produce no metallothionein, alcohol induced enlarged animal hearts. But when zinc was supplemented to the metallothionein-absent mice given alcohol, fibrosis was prevented. [Food & Agriculture Org. U.N. 2005]
In experimental studies it is surprising to find increased zinc protects the heart from damage when copper levels are depleted. Zinc activates the synthesis of metallothionein that in turn protects the heart during copper deficiency. [Journal Nutritional Biochemistry Nov 2007]
Metallothionein, the ubiquitous metal binding protein, requires 7 molecules of zinc to activate and capture potentially toxic metals like copper, mercury, cadmium and lead.
Low zinc intake results in weak metallothionein action. Excessively high-dose zinc given rapidly can theoretically induce too much metallothionein, which will mop up other heavy metals but also deplete zinc in their disposal. Because of this, a slow increase in zinc intake is advised by Dr. William Walsh of the Walsh Institute. [Walsh Institute]
It is no surprise to learn that unstable arterial plaque may trigger local metallothionein proteins as a protective factor that substitutes for zinc in the plaque area. [Current Medical Research Opinion March 2007]
Another important mineral in the prevention of atherosclerosis may be selenium. Selenium increases the release of zinc from metallothionein. [Current Pharmaceutical Design 2008] A dietary shortage of selenium might explain why high-dose zinc studies often fail to lower arterial plaque.
It makes sense that as humans age and zinc absorption declines and inflammation increases, atherosclerosis accelerates. [Ageing Research Review Dec 2008]
Low-grade inflammation can trigger compensating protective metallothionein, which sequesters zinc and limits its bioavailability. This explains zinc deficiency syndromes in old age, particularly atherosclerosis. [Annals New York Academy Science 2007]
Omeprazole (Prilosec) is a common antacid used to control heartburn symptoms. Omeprazole has been found to lower blood serum zinc levels. [Journal Trace Element Medicine Biology Oct 2010]
Of acute interest is the recent revelation that high homocysteine levels in the blood circulation impair the protective properties of zinc-controlling metallothionein and result in increased free (unbound) zinc. Homocysteine is an undesirable blood protein. Homocysteine targets metallothionein, which provides a plausible explanation as to why elevated homocysteine levels promote atherosclerosis. [Arteriosclerosis, Thrombosis & Vascular Biology, page 8, 2007; page 49.] B vitamins (B9 folic acid, B6 and B12) reduce homocysteine.
A dietary factor called phytate (phytic acid or IP6) is said to impair the absorption of zinc.
Researchers found a high ratio of phytate IP6 over zinc results in increased risk for atherosclerosis in men by up to 258%. The intake of IP6 ranged from 435 to 738 mg/day and the intake of zinc 6.1 to 7.3 mg/day. [PLoS One 2013]
It is difficult to interpret the above report because dietary IP6 intake was deemed to be high but a plant food diet provides ~1500 mg of IP6 per day. Animals fed IP6 have strikingly reduced calcification of their aortas (first blood vessel outside the heart). [Frontiers Bioscience May 1, 2008] IP6 also binds to iron.
IP6 is reported to lower serum cholesterol levels and favorably alter the zinc/copper ratio. [Anticancer Research Sept-Oct 1999]
IP6 phytate may be getting a bum rap. It has been observed that vegetarians who consume extremely high amounts of IP6 phytate have normal blood serum zinc levels even thou consumption of zinc is relatively low. [Journal Nutrition 1984; Journal American Dietetic Association March 1978]
Polyphenols such as those found in red wine (resveratrol, quercetin) stimulate the uptake of zinc by metallothionein while IP6 (phytic acid) limits metallothionein uptake of zinc making it more bioavailable. [Journal Food Science 2010]
The absorption rate for zinc from food ranges from 20-40%. [University Maryland]
Vitamin B6 facilitates absorption of both zinc and copper. [International Journal Vitamin Nutrition Research 1997]
Zinc is bound to various carriers by electron attraction (valence). Zinc dietary supplements provide varying amounts of elemental zinc, as follows:
Zinc acetate, 30% elemental
Zinc gluconate, 14.3% elemental
Zinc sulfate, 23% elemental (poorly absorbed)
Zinc citrate, 34% elemental
Zinc glycinate, 25% elemental
Zinc carnosine, 22% elemental (often used to quell H. pylori)
Zinc monomethionine, 21% elemental
Zinc picolinate, 23% elemental (superior absorption offset by increased elimination) [National Academy Press]
Zinc oxide, 80% elemental (but insoluble in water) [PubChem]
So what are we to conclude? High/low dose copper, high/low dose zinc foster/don’t foster the development of atherosclerotic plaques in coronary arteries. What are we to deduce after four-plus decades of confusing research?
Much of the scientific confusion emanates from animal research where non-physiological and frankly impractical doses of dietary fat or minerals are given to animals to produce a desired effect. Just how translatable the findings of these reports are to human health is debatable.
The preponderance of the science suggests weak zinc levels in relation to copper foster the onset of atherosclerosis.
However, it needs to be said that this more likely applies to iron-overloaded adults than growing children who generally are iron deprived because of their iron demand to make new red blood cells during childhood growth. As previously stated, zinc eradicates atherosclerotic plaque by deplacement of iron
It turns out George A Eby, a self-educated pharmacologist and world expert in zinc nutriture may have the needed answers.
Over a decade ago Eby along with Dr. William W. Halcomb wrote a landmark paper entitled: “High-dose zinc to terminate angina pectoris: a review and hypothesis for action by ICAM inhibition. [Medical Hypotheses 2006]
Eby and Halcomb write that among patients with angina chest pain there was no difference in blood serum concentrations of zinc, nor red blood cell zinc or hair analysis, whether they had accompanying atherosclerosis or not. But there was a major difference in zinc concentration in the aorta, the first blood vessel outside the heart (40.6 parts per million in healthy aorta, 19.4 in atherosclerotic aortas).
The provision of high-dose zinc raised blood serum zinc levels from 95 micrograms per deciliter of blood to 177 micrograms, which resulted in objective improvements in 12 of 16 test subjects.
Eby and Holcomb wrote that zinc prevents oxidation (hardening) of LDL cholesterol and halts the main mechanism of atherosclerosis. Zinc also blocks calcium and its stiffening of arteries.
They hypothesized that a therapeutic mega-dose of zinc (300 milligrams) per day would induce the slow release of LDL from cardiac tissues thus flushing it into the blood serum where it can be readily observed. These bold researchers wrote:
In stark contrast to current practice, high dose zinc should be considered as basic in the strategy of prophylaxis and therapy of the atherosclerosis process to terminate angina pectoris and restore youthful cardiac function.
Eby and Holcomb assert that low-dose or poorly available zinc compounds (zinc oxide) do not reduce LDL cholesterol whereas high-dose zinc (50-300 mg/day) decreases HDL and increases LDL cholesterol in the blood circulation. You may need to read this again. LDL blood levels increase with mega-dose zinc. The elevated LDL blood level is due to the disposal of LDL. It is exiting the body.
Eby & Holcomb turn zinc research upside down. At least in regard to mega-dose zinc, high LDL cholesterol blood levels after zinc therapy represents the disposal of cholesterol, not excessive blood levels of cholesterol. This changes the conclusions drawn from all of the prior zinc studies.
Eby and Holcomb report of a patient with chronic angina of 15 years duration who experienced vanishing angina without the need for any medication. A similar result was experienced with another angina sufferer.
Eby and Holcomb refer back to a report published in 1968 that noted the administration of zinc sulfate was beneficial to patients with inoperable severely symptomatic atherosclerosis. [Trace Substances in Environmental Health, 2nd conference proceedings, 1967-68] Another researcher reported similar results in 1971. [Trace Elements Human & Animal Nutrition, Academic Press, 1971]
Eby and Holcomb also point to a 1980 study of workers industrially exposed to zinc and other minerals. Environmental exposure to zinc in mines in Poland resulted in a 40% reduction in the incidence of physical exertion angina. [Coronary Diseases, Przegl Lek 1980]
Similarly, patients taking 80 mg zinc/day for macular degeneration experienced a 27% decline in mortality. [Archives Ophthalmology May 2004]
These investigators suggested caution when taking mega-dose zinc. Therapy should not extend beyond 14 days and supplemental copper may be wise to prevent weakening (aneurysms) in arterial walls. Insoluble zinc oxide should be avoided. Other more soluble forms of zinc should be employed.
Copper pipes in plumbing began to be routinely installed in American homes in the 1960s. [Home Instructions] The World Health Organization recommendation is that copper in drinking water not exceed 2.0 milligrams per liter. [Environmental Health Perspectives 2004] The U.S. EPA maximum contaminant level goal for copper is (1,300 parts per billion (1.3 mg/liter) To picture this amount in your mind, one milligram/liter is equal to 4.5 drops in a 55-gallon barrel of water. [National Sanitation Foundation] Copper from plumbing may have altered the zinc/copper ratio in the diet.
The widespread number of plagues released by zinc deficiency in modern times, which include autoimmune disorders, childhood behavior and learning problems (autism, dyslexia, etc.), weak immunity and poor response to vaccines, premature aging, skin problems, and many other preventable human maladies, appear to have been induced by a change in zinc nutriture at some point in time.
In the search for an environmental or dietary culprit, consumption of high fructose corn syrup, which came into common use beginning in the late 1970s and is widely consumed in soda pop, can lead to zinc losses. [Behavior Brain Function Oct 27, 2009] High fructose corn syrup is identified as a zinc/zinc binder (metallothionein) disruptor. [Clinical Epigenetics April 10, 2012]
Bottom line: Modern medicine has kept the zinc cure for atherosclerosis hidden in the closet for over 40 years. In the adult years, particularly for males over age 40 and females approaching menopause, zinc supplementation is wise in order to maintain healthy arteries. Suggested dosage is 25-30 mg/day with accompanying vitamin B6 (no more than 25 mg) to increase absorption and 200 mcg of selenium to facilitate release of zinc from its binding protein (metallothionein). Zinc oxide, the most economical form of zinc, is largely insoluble and other forms of supplemental zinc should be used.
ATHEROSCLEROSIS |
||
|---|---|---|
| STATIN DRUGS | ZINC | |
| Type | Synthetic liver toxin | Natural trace mineral |
| Method of control | Reduces cholesterol synthesis in the liver (total and LDL) | Prevents cholesterol from oxidizing (hardening) in adults |
| Secondary action | Promotes coronary artery calcification | Reduces coronary artery calcification |
| Impact on gut bacteria | Cholesterol-lowering effect depends upon gut bacteria (bile acids) | Zinc deficiency reduces gut bacteria diversity |
| Co-factors | Zinc, copper & magnesium may decrease statin blood levels. Grapefruit juice may inhibit breakdown of statins and increase statin drug toxicity | Vitamin B6- improves zinc absorption Selenium – increases release of zinc from binding protein (metallothionein) |
| Potential side effects | Severe muscle pain; depletes coenzyme Q10; liver damage, kidney failure, mental confusion, diabetes, cataracts | Zinc/copper imbalance (?) Metallic taste |
Savvy readers may inquire about copper and its role in cardiac health. Copper is not always problematic in heart disease. Copper deficiency is alleged to be a primary cause of age-related heart failure. But heart failure is not atherosclerosis. Ischemic (oxygen deprived) heart disease is the leading cause of death in middle age and is a major obstacle to achieving longevity.
There are numerous similarities between animals deficient in copper and people with ischemic heart disease. No other nutritional insult has produced such a demonstrable effect in experiments with animals; men fed diets abjectly low in copper have increased cholesterol, decreased glucose tolerance, and abnormal electrocardiograms. The process that results in ischemic heart disease is remarkably similar to that of copper deficiency.
More features of the etiology, pathogenesis, and pathophysiology of ischemic heart disease (not atherosclerosis) can be explained in terms of copper deficiency than can be explained by any other environmental insult. [Clinical Geriatric Medicine May 1987]
There is no question that frank copper depletion can result in heart failure by virtue of copper’s ability to support connective tissue. [Acta Physiologica Hungary 1994] Copper deficient diets in animals produces heart disease with accompanying elevation of blood serum cholesterol. [Biological Trace Element Research 2000] Copper deprived animals develop enlarged hearts. [American Journal Clinical Nutrition Dec 1993]
But heart failure is not atherosclerosis, which occurs in the inner lining of the arteries.
The provision of 10 milligrams of copper daily has not been shown to alter circulating cholesterol levels. [American Journal Clinical Nutrition Oct 1985]
But supplemental zinc can also be therapeutic for heart failure as well. When oxygen-deprived rodent hearts are injected with a zinc chelator (binder) they exhibit worse outcomes but zinc supplementation abolished the diminished cardiac function. [PLoS One Dec 15, 2016] Obviously, in cases of ischemic heart disease both copper and zinc are needed. ©2017 Bill Sardi, Knowledge of Health, Inc.
Posted in Dietary Supplements, Heart ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105