
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted February 2, 2015: by Bill Sardi
Delivered at the Sixtieth Annual Awards Dinner, National Health Federation
Woodland Hills, California, January 31, 2015
Public speaking coaches suggest you size up your audience before you deliver a speech. I’m told there are three ways to segment an audience; those who already embrace what I have to say; those who stand in the middle and need further convincing and those who oppose or disagree with what I have to say. I’m told those who oppose or disagree will not move all the way to embracing my thoughts, that the best I can expect is for them to move towards the middle and those in the middle move towards what I am going to suggest here tonight.
Now I have a problem because my assessment of this audience is either that they embrace alternative medicine and some of its obvious misdirection, or they embrace conventional medicine and all of its deadly trappings, or that they embrace parts of both which is practically where most people stand. The problem is, what if both are on the wrong track? Just how am I going to address such an audience?
In the next few minutes I am going to tell you that cancer has been cured and how you can do that without any hand holding, both with and without the use of conventional medicines. That should surely be the way to win over a bipolar audience such as this. But sadly, it won’t.
I am going to tell you that we have met the outer limits of what can be accomplished to prevent and cure cancer because in satisfying your proclivity towards conventional or alternative medicine I am still butting up against the greatest tool modern medicine uses in its deadly quest to control your mind and your healthcare decisions — FEAR.
Gripped with the fear of the fresh diagnosis of cancer what will you elect to do? I can tell you right now but I will save it for the end.
I just may demolish your closely held beliefs in alternative therapies – namely that alkaline diets cure cancer.
Here are the lines of evidence that alkalinity does not prevent or cure cancer.
Furthermore, I ask those who believe alkaline diets prevent cancer if they believe probiotic “friendly bacteria” such as acidophilus should be supplemented in the diet? Most respond positively. Yet acidophilus (its first four letters spelled out are A-C-I-D) is acid-forming bacteria.
Now, are you ready to hiss and throw me out of this conclave before I go any farther? It’s outrageous to believe I know what the cure for cancer is, after all, where is my Mayo Clinic diploma? I really have a lot of convincing to do get you to believe that in the next few minutes.
In the 1930s it was Otto Warburg who won two Nobel Prizes for his discovery that cancer cells convert from using oxygen to sugar for energy.4 There is always some “sugar burning” going on, but cancer cells generate up to 60% of their energy from sugar rather than ~5% in healthy cells.
By the way, because cancer cells utilize sugar for energy they expel lactic acid, and that is how the alkaline theory of cancer got started in the wrong direction. The acid is expelled outside of the cancer cell.
Indeed, the very way cancer is detected in this modern era is to image tumors using PET scan technology where radioactive sugar is instilled and the sugar is immediately attracted to feed the fast-growing ball of cancer cells wherever they may be, and then visualized on the PET scan.5 The cancer industry certainly knows sugar feeds cancer.
With recognition that changes in cell metabolism define the difference between healthy and malignant cells it is shameful that greater interest in cancer cell metabolism hasn’t been forthcoming sooner.6 An article in the Journal of the National Cancer Institute said the Warburg Effect is experiencing a renaissance. And that report was published a decade ago.7
All of the accumulated knowledge to date involving cancer cell metabolism strongly suggests limitation of refined sugars to control tumor cell growth.8
The particular type of sugar consumed may influence cancer risk. A recent study is instructive. Six of ten mice fed a diet rich in high fructose corn syrup developed liver tumors over a 12-month period of time versus zero tumors in mice fed a normal diet.9
But for inexplicable reasons, limitation of dietary sugar is not in the average oncologist’s armamentarium.
From an experiment conducted in 1909 that demonstrated the growth of implanted tumors was inhibited by underfeeding mice, to reduction in the recurrence of tumors from 82% in fully-fed mice to only 28% in underfed mice in an experiment conducted in 1926, it has been widely known that diet can control cancer.
Another experiment showed that a limited calorie diet combined with high-fat intake reduced tumor incidence from 73% to just 7%.
We’ve known for over 100 years that diets can control cancer yet there is no recommended diet for cancer patients.10
A report in the journal The Oncologist suggests that dietary restriction or intermittent fasting “may be a potent supportive intervention for patients undergoing standard cancer treatment.”11 But is there a cancer patient that ever hears of this?
Inexplicably, the dietary recommendation for cancer patients receiving chemotherapy, as described by the American Cancer Society, is to increase calorie and protein intake.12
Ketone bodies inhibit malignant cell growth.13
The original ketogenic diet was designed by Dr. Russell Wilder in 1924 to treat epilepsy. It is a diet high in fat, adequate in protein and low in carbohydrates.
There already is a ketogenic medical food called KETO-CAL14, a nutritional food that is 1.6% carbohydrate and 90% fat used to treat childhood epilepsy that has been shown to reduce brain tumors in animals by 35-65%. Good God, we already have a nutritional-based cure for cancer.
All three dietary approaches, calorie restriction (fasting) or a low carbohydrate diet or a ketogenic diet, reduce blood glucose levels that tumor cells depend upon for survival.
The use of a low-carbohydrate (no bread, no rice, no pasta), or calorie-restricted and/or ketogenic diet (low calories, high fat) decreases the growth of cancer by 15-30% in animals. The remaining growth depends on glucose formed by the liver.
Diabetes is common among patients with cancer.15
An interesting study of 119 breast cancer patients found 65.5% had diabetes or pre-diabetes with 80% of these cases of diabetes being previously undiagnosed.16
In older women there is a strong connection between breast cancer mortality and sugar consumption.17
It is instructive to learn that in the animal lab 50% of mice fed a carbohydrate-rich western diet exhibit tumors by age 1 whereas no tumors are detected in mice fed a low carbohydrate diet.
Now it should come as no surprise to learn that the anti-diabetic drug metformin is being re-purposed as an anti-cancer drug.18
The anti-diabetic drug metformin works to reduce blood sugar levels by reducing glucose production in the liver. This suggests limited sugar-carbohydrate diets combined with inhibition of glucose synthesis from the liver would be the most appropriate anti-cancer therapy.19
Does metformin do more than shrink tumors? Does it reduce mortality and save lives? For comparison, chemotherapy drugs gain approval from the FDA if they shrink tumors by 50% even though they don’t prolong survival. The most recent study indicates metformin does indeed reduce mortality from cancer and from all-causes by about 25%.20
Metformin first gained approval by the FDA in 1957 for the treatment of adult-onset diabetes. In 1971 the idea that metformin may be a promising anti-cancer drug was first proposed and subsequent animal experiments in that same decade confirmed that notion. A report published in Science magazine in 2012 states that metformin may have saved more people from cancer death than any drug in history as some 120 million prescriptions are written for it annually.21
So let’s go to our doctor and demand we get an Rx for metformin. But wait. We know modern medicine has dragged its feet for over a century on the connection between diet and cancer and for over 80 years since the discovery by Otto Warburg in Germany that cancer cells thrive on sugar; and since 1971 when it was first realized metformin reduces cancer growth and mortality. Why are we going back and asking our doctors for metformin when they have lost all level of trust?
But what if we, for many reasons, don’t want a synthetic drug to treat our cancer? There is a natural molecule for you.
Metformin genetically produces its anti-cancer effects primarily by exerting its influence over a key enzyme, AMPK.22
And it turns out that resveratrol, known as a red wine molecule, has been found to increase AMPK 200 times better than metformin.
A remarkable comparison was performed in the animal lab between metformin, the anti-diabetic drug, and resveratrol, the red wine molecule. At a 30 times lower dose, resveratrol outperformed metformin, demonstrably reduced blood sugar levels, improved the ability of insulin to enter cells and produce energy and activated more internal antioxidant enzymes as well as restored vitamin C levels to normal better than metformin.23
Modern medicine is ignoring resveratrol, but you don’t have to.
Resveratrol also turns off the cancer switch.
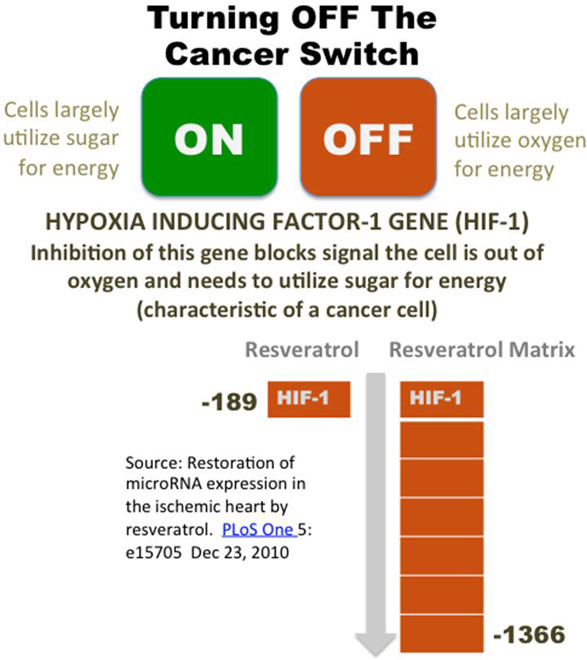
The switch that causes healthy cells to convert to using sugar for energy is called hypoxia inducing factor-1 or HIF-1 for short. There is compelling evidence that hypoxia inducing factor-1 (HIF-1) is that very switch that signals cells to utilize sugar for energy.24,25,26,27,28,29
But what would happen if we blocked that cell signal? What if we shut off the HIF-1 protein from being produced? Cells might actually be oxygen deprived, but if the HIF-1 signal is not sent, cells would not convert to utilization of sugar for energy.
Also HIF-1 inhibition blocks the development of new blood vessels that facilitate the delivery of sugars and other nutrients to the tumor site.
The most profound HIF-1 inhibitor, pharmaceutical or nutriceutical, is a matrix of natural molecules called polyphenols available as a propriety dietary supplement, a proprietary formula I confess I have a financial interest in. In research conducted by National Institutes of Health researchers report this nutraceutical was found to down-regulate genes that control HIF-1 by -1366-fold in rodent heart tissues. This was compared to plain resveratrol -189 fold.30 The cancer switch can be demonstrably turned off by an off-the-shelf molecule – resveratrol and more so when combined with other similar molecules.
The scientific literature points to combination therapy, low sugar and low carbohydrate diets combined with drugs and/or nutraceuticals to successfully subdue cancer.
Oncologists only mention in passing that there are no cures for cancer and in fact, cancer cells are only temporarily killed off with chemotherapy or radiation. Since treatment is spaced out to allow for recovery, during these intervals cancer cells repopulate.32
Seventy-percent of cancers are solid tumors which radiation or chemotherapy cannot penetrate.33 Chemotherapy inevitably results in cancer treatment resistance and destroys the immune system. Modern cancer treatment is largely an exercise in futility.
Infusion of chemotherapy agents in the oncologist’s office, which by one report only contribute to ~2% of the cancer cures34, generates 80% of an oncologist’s income.35 Any therapy that would interrupt that income stream would likely be ignored or rejected outright.
Nothing may ever be allowed to change in the cancer treatment arena. But that doesn’t mean you need to be a victim of cancer and/or be duped by the cancer treatment industry.
Will anything that I said tonight change the way you practically address your diet or alter your health decisions? That is not likely.
A long-term study in Canada showed that patients who elected to undergo cancer treatment achieved a median survival of only 9-months over patients who refused to undergo radiation, surgery or chemotherapy.36
Do you think that you would stand a good chance of living more than 9 months longer by adhering to what you have learned here tonight? Do you think that a low sugar/carbohydrate diet combined with a drug like metformin or a molecule like resveratrol would prolong life by 9 months without all the pain, suffering, anguish and financial ruin that results from modern cancer treatment?
It was John Ely PhD who had shown in the animal lab that only 1 in 20 mice (5%) fed a low-sugar died expired from implanted breast tumors whereas 16 of 24 mice (66%) fed a high-sugar and carbohydrate diet failed to survive37, ventured to place two end-stage terminal breast cancer patients on a low-sugar/ low carbohydrate diet combined with oral vitamin C. Each subject shed 50 pounds and lived 11 and 13 years respectively.38
So what are you going to tell others about what you heard tonight? You may tell others you heard some homeopathic lecturer talk about sugar and cancer at a dinner party and you decided to forgo dessert. You are stymied. You don’t know what to do with the information that has just been delivered to you. You, you want to check with your doctor first. You need to hear this from others before you believe it. Why doesn’t my doctor tell me this, you ask? Yes, why doesn’t he?
You see, you have never made an independent health decision in your lifetime and now you are being asked to do that in regard to a mortal disease. You are paralyzed by the thought of making the wrong decision.
If your mother has cancer and you attempt to share this information with her to forgo chemotherapy, your relatives will secret her away for a second opinion with an oncologist and you won’t be able to stand up to them. They have the doctors and all that medical technology on their side and all you have is a few herbs and a diet in their place.
In summary, if you prefer conventional medicine and you or a loved one are diagnosed with cancer or desire to prevent recurrence of cancer you might consult with a licensed physician about a prescription for the anti-diabetic medicine metformin.
If you adamantly have camped yourself away from using any conventional cancer treatment and are looking for a natural remedy, you might start with resveratrol in modest doses (no more than 350 milligrams/day). If you already take metformin, you can take resveratrol with it to potentiate its action.
If you absolutely don’t want anything to do with pills, you can start with a low-sugar/ low-carbohydrate diet.
So where did I just leave my audience – perplexed, paralyzed, frightened, pulled in two directions, pitted against family members and doctors, feeling they face the rest of life without ever having a chocolate chip cookie again, feeling exploited by the cancer treatment industry, and needing validation from other sources? Shall we muscle test the ideas presented here? You will have to sort it out from here on your own.
I often ask myself why I beat myself up attempting to reach out to people who have no ears to hear? My message of hope is trumped by white coated-doctors with Mayo Clinic diplomas. But how can they say it is unproven, especially when chemotherapy and radiation treatment have been disproven?39 And with that said, why don’t we take care of all the tension I have just created and have an extra dessert?
© 2015 Bill Sardi, Knowledge of Health, Inc.
References
Posted in Cancer ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105