
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted March 16, 2020: by Bill Sardi
I don’t fear a virus that is allegedly infecting and killing as much as I do politically induced panic. There are so many mixed messages based upon faulty if not contrived and outright fraudulent data it is difficult to short out and draw any conclusion from this so-called pandemic. And now, as if there wasn’t enough confusion, we have government permission to pray but we can’t go to church (ban on assembly in large groups)! More about that at the end of this report.
Under the conjured-up fear of death, world populations have willingly complied with political mandates to lockdown and self-quarantine indoors and avoid contact with others, essentially freezing economies and further worsening a respiratory disease season that is largely defined by a lack of sunshine vitamin D in winter months.
Health authorities should know coronaviruses come in November-December and decline in April and May (see chart below). Regardless of testing or treatment, as the earth tilts back towards the sun in spring and summer the coronavirus outbreak should subside. If it doesn’t, one should suspect falsified science and fake news reporting.
Coronavirus was always in circulation but human immune systems are weak in winter due to a lack of sunshine vitamin D, a preventive modern medicine chooses to ignore.
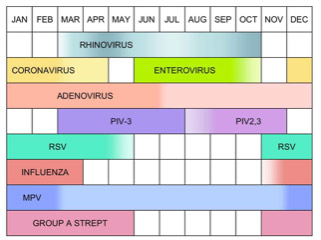
Seasonal variation of selected upper respiratory tract infection pathogens. PIV is parainfluenza virus, RSV is respiratory syncytial virus, MPV is metapneumovirus, and Group A strept is group A streptococcal disease
Political posturing has entered the discussion over how to handle the coronavirus epidemic. With an anticipated month off work, one wonders how Americans are going to pay their taxes on April 15. Critics of a proposed payroll tax cut for the remainder of the year issued the usual opposition from the other side of the political aisle asserting such a measure would only benefit the wealthy – – but those are the only people paying taxes (the bottom 45% of American households pay no federal taxes, though they do pay mandated payroll deductions for Medicare & Social Security).
Put yourself in the situation room. Here is what is known.
The US doesn’t have an adequate supply of test kits to confirm respiratory disease cases are COVID-19 coronavirus. What good would testing do? Treatment is not necessarily tailored to the type of virus detected and sunlight cures all infectious respiratory tract diseases.
It could be presumed that laboratory-confirmed infection with survival would indicate an individual has developed natural antibodies and would therefore not benefit from or need to be inoculated when a vaccine gains approval. However, the current COVID-19 test determines who is spreading the disease. A new test that measures whether adequate antibodies were produced would determine who, among the infected and certainly the uninfected, would benefit from future vaccination. Those individuals with sufficient antibodies would not benefit from vaccination. They have developed memory T-cells that afford long-term immunity. The CDC makes no mention of this side benefit from prior infection. And the CDC is likely planning universal mandated overvaccination.
Why the CDC released testing kits that provide faulty results (false positive and false negatives) goes unexplained. The labs the CDC dispatched the tests to detected the problem, not the CDC. How could labs detect the flawed test kits and not the CDC?
More befuddling, a recent report indicates infected patients may exhibit positive testing days after hospital discharge. Then do these people have to remain under quarantine?
It is difficult to fashion a rationale how testing is going to slow rates of infection. In the United Kingdom (UK), 20,388 people were tested to find 163 cases of COVID-19 coronavirus infection (less than 1% infection rate). No mention is made what brought the other 20,225 to the clinic or hospital for examination?
Congress just passed legislation for free testing. The masses are mindlessly going to clamor for the test. Politicians are already making noise the poor should have equal access to testing.
Rather, testing should be targeted at high-risk groups (mostly the aged) as infection rates among the young and healthy are nil. And just precisely what does a doctor do with an 80-year old with no symptoms who tests positive for COVID-19?
Early testing and quarantine in South Korea are said to have resulted in a very, very low (7/10ths of 1%) mortality rate among those infected (51 deaths among 7.478 infections as of March 9), compared to 3.4% in Wuhan, China. However, careful review of this report reveals this low death rate is not attributed to testing or treatment but rather the fact 63% of infected individuals were young, according to a report in Asia Times. Cases of lung infection in younger adults suggest tuberculosis, not coronavirus.
Testing itself can falsely fan the flames of fear. As explained in a report in Science News, “If you’re going to test in a State that doesn’t have a coronavirus outbreak right now (3 States), with a specificity of 90% (specifically confirms COVID-19 and not some other virus is present), 10 out of 100 people are going to show up positive even though the coronavirus isn’t there yet.”
Nothing like spreading false panic. The CDC has been doing this with its false flu numbers for years. An authoritative report published in Epoch Times reveals out of 62,034 deaths in 2001 reported for influenza and pneumonia, only 18 cases of the flu were laboratory confirmed! This represents massive over-vaccination.
There is so much confusion over the flu versus flu-like illnesses that reporting from the CDC is like a hidden card trick.
To ensure there is enough flu going around, the FDA re-released nasally instilled FluMist which is known to facilitate shedding of viral particles and spread of infection. A CDC panel recommended Flu-Mist be withdrawn from use in 2016. Flumist was reported to be inferior to standard needle-instilled viral particles. A major problem is that Flumist sheds viral particles that may put immune compromised family members at risk for infection (a great way to start an adult epidemic from children to grandparents).
We don’t know whether people are dying of the seasonal flu, coronavirus, or something else (likely is Mycobacterium tuberculosis; which would likely infect younger Latino immigrants in the US with latent TB).
Coronavirus respiratory tract disease does not appear to be spreading into the community, though it may spread within a household where residents typically have similar risk factors (age, smoking, etc.).
As of Friday, March 13, 2020, The Centers for Disease Control reports 1629 infections and just 41 COVID-19 deaths in the US. Based on these miniscule infection and death rate numbers the US was placed on lockdown and incoming international travel banned.
For comparison, the CDC reports the 2019-2020 seasonal flu has produced 36 million “flu-like” illnesses, 370,000 hospitalizations and 22,000 deaths, but no lockdown for that reason this year or in prior years. (These are not true numbers.)
Of course, what is revealed is those flu deaths are over-reported in order to scare the public into getting flu shots. What does this say about the trustworthiness of the CDC?
This flu season the CDC has distributed over 174 million doses of flu vaccine. In past years the effectiveness of the flu vaccine has been miserable.
The 2019-2020 cumulative rate for hospitalization due to influenza is 61.6 per 100,000 is far under the hospitalization rate for the flu in 2017-2018 (more than 100 per 100,000). No quarantine then either.
The CDC combines pneumonia and influenza deaths to create a seemingly dire threat that induces fears that prod the public to vaccinate.
The CDC says 129 of these COVID-19 coronavirus cases are considered “close contact” (likely among family members who have same risk factors (age, smoking, etc.) and 138 were “travel related” (returnees from China and from a cruise ship), with 1362 “under investigation” (but no adequate way to confirm by laboratory testing). In fact, the CDC posted the following asterisk under its data page:
* Data include both confirmed and presumptive positive cases of COVID-19 reported to CDC or tested at CDC since January 21, 2020, with the exception of testing results for persons repatriated to the United States from Wuhan, China and Japan.
These 1362 cases may be nothing more than normally-occurring flu infections. They may be false-positives.
There were 3 cases of infection reported for Americans repatriated from Wuhan, China and 46 cases from the Diamond Princess Cruise Ship, where authorities quarantined vacation travelers and made the outbreak worse by holding people in close quarters and in their dark sunshine-less cabins.
The CDC is reporting a broad range of estimated cases in each state, for example 201-500 in Washington State and 201 to 500 in New York State. Translation: it’s a guessing game. Politicians (governors) are doing the reporting of these State infection rates.
Strangely, no (zero) cases are reported for Idaho, Alabama or West Virginia (so-called RED states).
The decision to block travel from Europe to the US appears to have been based on the situation in Italy, where health authorities there say they were mistaken in not closing the borders earlier.
But Italy appears to have increased mortal respiratory tract disease among 18-44 year-olds, which would point to immigrants in Northern Italy who likely have latent tuberculosis, while its senior adult population appears to have normal seasonal flu that sometimes has mortal consequences. Italy was in a battle to control tuberculosis cases long prior to this recent spate of deaths.
If health authorities in the U.S. would have any rationale to close borders it would be the southern border of the US where immigrants with latent (dormant) TB enter the US every day and many are already here in the US experiencing eruption of latent TB with lung infection that mimics the flu or COVID-19 coronavirus infection.
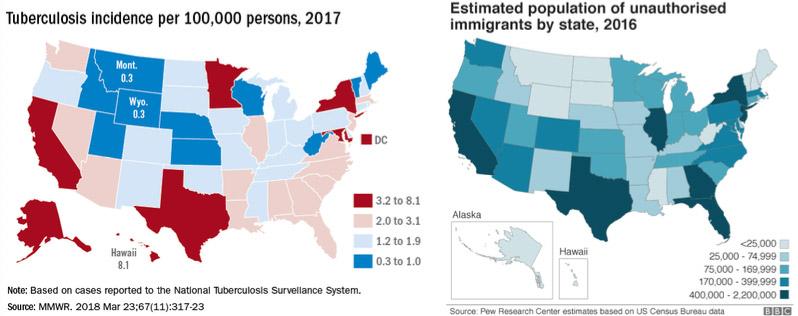
The US tuberculosis map appears similar to the number of immigrants in the US.
Furthermore, cases of tuberculosis appear to overlap immigrant population and cases of COVID-19 coronavirus appear to overlap the reported cases of tuberculosis (see maps above and below).
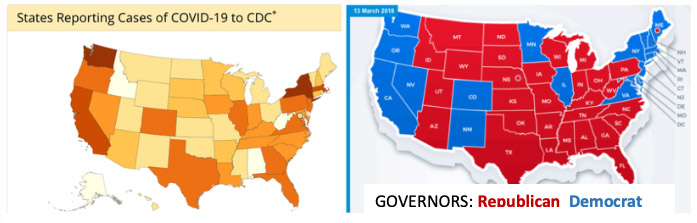
Strangely, prevalence of cases or suspected cases of COVID-19 coronavirus infection appear to follow along political lines, except for Texas, Arizona and Florida on the southern border where cases of respiratory infection among migrants are more likely to be latent eruptions of tuberculosis rather than COVID-19
For unexplained reasons, political party affiliation appears to be strongly associated with reported cases of COVID-19 coronavirus. It appears there are more reported cases of COVID-19 coronavirus in so-called BLUE States with Democrat Party Governors than RED States with Republican Party governors. Political persuasion predominates for reported cases of this disease. But given there is no reliable test, the question begs to be asked: is over-reporting for COVID-19 infection a politically-motivated agenda in Democrat-governed States?
An epidemiologist concedes all that testing may accomplish is catch false positives (individuals who aren’t infected but the test errantly says they are), which will be indiscriminately reported by a politically slanted news media.
Laurie Garrett, formerly a fellow at the Council on Foreign Relations who now works as a journalist for Newsday, in her report entitled “Trump has sabotaged America’s coronavirus response” published at Foreign Policy, takes a swipe at the White House for budget cuts.
The CDC is smarting from Trump administration budget cuts from $11.5 billion to $7.7 billion in fiscal year 2020.
Garrett writes another scathing, finger-pointing report posted online, entitled: “US COVID-19 CASES NOW SPREADING DUE TO TRUMP’S TESTING RESTRICTIONS AND DISMANTLING OF PANDEMIC RESPONSE TEAMS. Testing would not prevent the spread of the virus however (refer to experience in South Korea earlier in this report).
Is the CDC striking back at budget cuts, releasing flawed test kits, reporting false positives, over-reporting mortality rates, with hidden political motives? And placing the whole world on hold?
Nothing like igniting a false epidemic built on false positive testing and attributing deaths among vulnerable 80-year-olds to COVID-19 coronavirus when ANY infectious pathogen could be life threatening at that age.
There is no unbiased news media to point out the many discrepancies in this unprecedented epidemic. News agencies depend on government for news. They are not going to challenge the main source of news which is the lifeline of their business. And the public is fully aware news agencies are politically biased against the current administration in Washington DC.
When the primary association for reported cases of COVID-19 coronavirus infection is the political party affiliation that controls State governance, something is amiss.
According to a report published in The New York Times, COVID-19 coronavirus was spreading throughout the US for weeks prior to the announced epidemic. A spreading epidemic appears to have been declared at a politically chosen time.
Someone said never let a crisis go to waste. What is the end-game here?
Dr. Anthony Fauci, director of the National Institute of Allergy & Infectious Disease has been quoted to say: COVID-19 is “ten times more lethal than seasonal flu.” According to data provided by the CDC itself, that is a false statement.
There may be some naïve Americans who believe ruses like this, but there are many more Americans, who like the government’s assertion that Arabic terrorists in Afghanistan were responsible for 9-11, don’t believe it and know our government is behind it.
I think many Americans know this viral epidemic is not real, but the panic-buying is. That the data behind this coronavirus is flawed and the epidemic contrived.
I think politicians know that too, but must pretend it is for real to sustain their political lives.
I think that this is not a question of whether hand washing or mask wearing effectively prevents the spread of infection. I think this is a test of our obedience and willingness to comply. The false god of government must be obeyed. Resist social pressure to vaccinate your family against coronavirus or your neighbors may burn your house down.
Like a solution to global warming is to stop using plastic straws or to curb the use of drinking water in restaurants, or to keep our tires filled with air so we don’t need so much oil, which are largely meaningless in the larger scheme of things, we are pressured to make hand washing and mask wearing social norms, what are called mores — practices that are morally acceptable or unacceptable within a culture.
By being forced to disband (self-quarantine) and not congregate, we can’t mount up opposition to government. We may now have to tune in to an online church service instead of attending a synagogue or church, or take a school class from home. But then we won’t be talking to each other. The churches and synagogues may be the last line of resistance in a covert effort to take away the right to assemble, banned under the guise of halting the spread of infectious disease.
The medium is the message. The public narrative is easier to control this way. That is the possible end game. Profiteering along the way and mandates and/or social pressure for universal vaccination is a side bar in the quest to control the public’s mind.
Posted in Coronavirus, Uncategorized ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105