
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted June 20, 2019: by Bill Sardi
If you want to avert the development of a sight-robbing disease called macular degeneration you are going to have to step outside modern medicine. Eye doctors only have treatment but no prevention for this dastardly eye disease that robs senior adults of their central vision for reading, driving and watching TV.
Don’t both your eye doctor about this proposed vitamin cure for macular degeneration. Your eye doctor will demand a controlled human study before he/she prescribes a vitamin. There are no published human studies to confirm its safety and effectiveness and none are planned. So, it is unproven (but not disproven). You will just have to endure slow progressive loss of vision (dry macular degeneration) and hope you don’t develop the fast-progressive form (wet macular degeneration), which requires monthly needle injections directly into your eye(s) to avoid permanent loss of vision.
The National Eye Institute promotes a multi-nutrient formula called the AREDS formula (Age-Related Eye Disease) that barely slows the progression of this disease (you still are losing your sight). The AREDS formula does not benefit patients with early macular degeneration.
A simple vitamin cure for macular degeneration has eluded eye researchers for decades and now that the ophthalmic industry has come to rely on a multi-billion dollar income stream generated by 12 million worldwide annual needle injections of medicine (5.9 million U.S. 2016) directly into the eyes to stave off permanent loss of vision. There is little if any financial impetus to prevent or cure this disease. Would it be that modern medicine allows an eye disease to progress to precipitous loss of functional vision and then attempts to rescue vision only temporarily, requiring repeated treatment, rather than prevent the disease from occurring in the first place?
This eye disease is age-related, striking a significant portion of senior adults and robbing them of independent living in their retirement years. What is the initiating factor that brings on this devastating eye disease that robs older adults of their central vision?
The medical literature points to chronic insufficient supply of oxygen to the retina, which is (incorrectly) called ischemia (iss-keem-ee-ah), as the instigating factor in macular degeneration. This report makes a scientific argument that chronic ischemia initiates macular degeneration and is also the malevolent factor in the onset of a host of other eye disorders (glaucoma, macular edema, diabetic retinopathy, retinal vein occlusion and uveitis) as well as many non-ophthalmic maladies such as chronic obstructive pulmonary disease (COPD), dementia, angina, and Alzheimer’s disease.
Numerous researchers conclude that oxygen deprivation is the starting point for dry macular degeneration:
“Our research supports the association of ischemia with dry macular degeneration.” —British Journal Ophthalmology Aug. 2013
“All retinal nerve cells are most susceptible to ischemia.” — Annals Ophthalmology (Russian) May 2010
“Ischemia may play a central role (in macular degeneration).” — Progress in Retinal Eye Research Sept. 1999
One might say there is scientific consensus that oxygen deprivation is at the starting point for the disease.
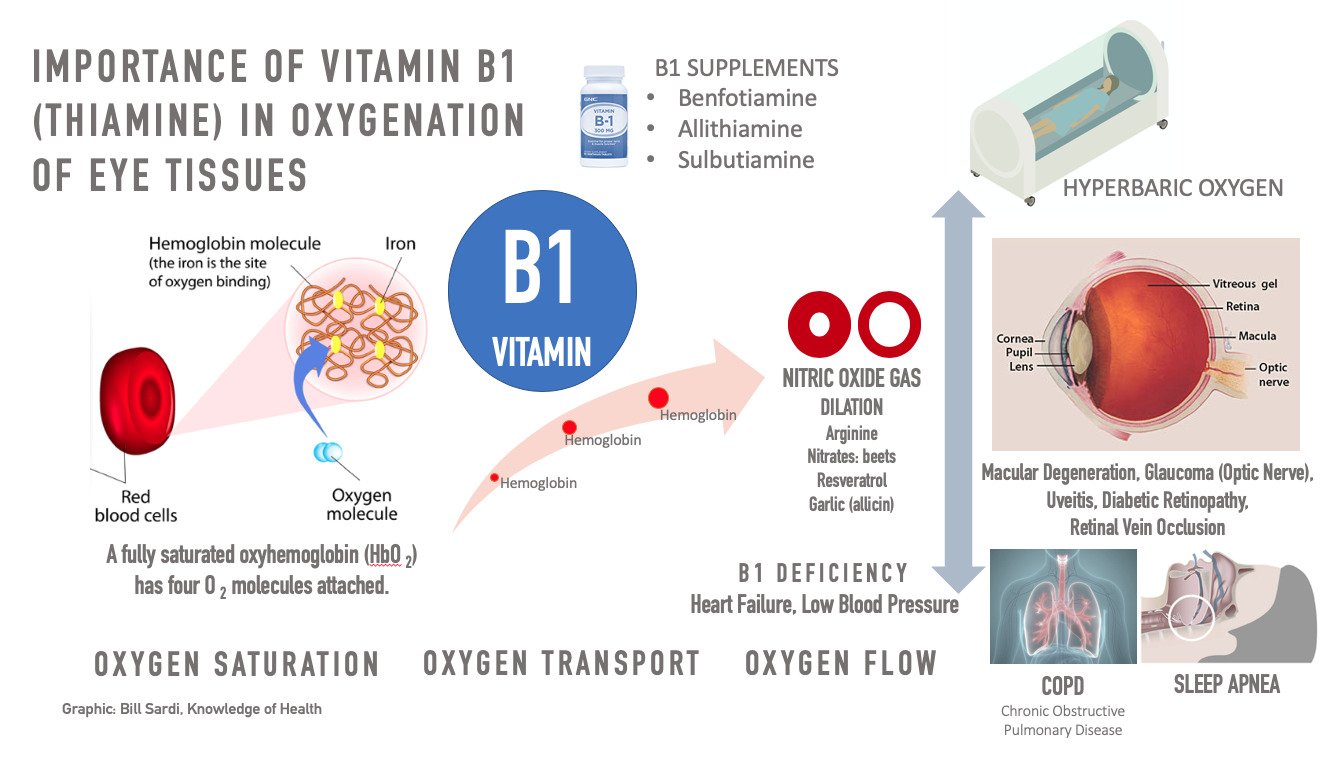
This report also reveals a single nutrient, thiamine (thii-ah-meen) vitamin B1, by virtue of its ability to facilitate the transport of oxygen on hemoglobin (the red oxygen-carrying pigment in red blood cells), as the antidote to eye, nerve, heart, brain and lung disorders.
By definition, ischemia is insufficient blood flow to provide adequate oxygenation to cells. Ischemia may then lead to tissue hypoxia (hi-pox-ee-ah), reduced oxygen, or anoxia (an-ox-ee-ah), which is absence of oxygen altogether.
However, these defined terms do not encompass what actually may be happening. It may not be impaired blood flow but rather impaired transport of oxygen to tissues that induces disease. This etiology is generally not considered in research papers.
Reduced tissue oxygenation is strongly implicated in the onset of macular degeneration. Impaired oxygen delivery can emanate from a deficiency of thiamine (vitamin B1) required for cell energy and oxygen delivery on hemoglobin.
To continue, an understanding of how the retina of the human eye is organized is necessary to understand how macular degeneration gets started.
The retina is organized from back to front as follows:
Back of Eyes
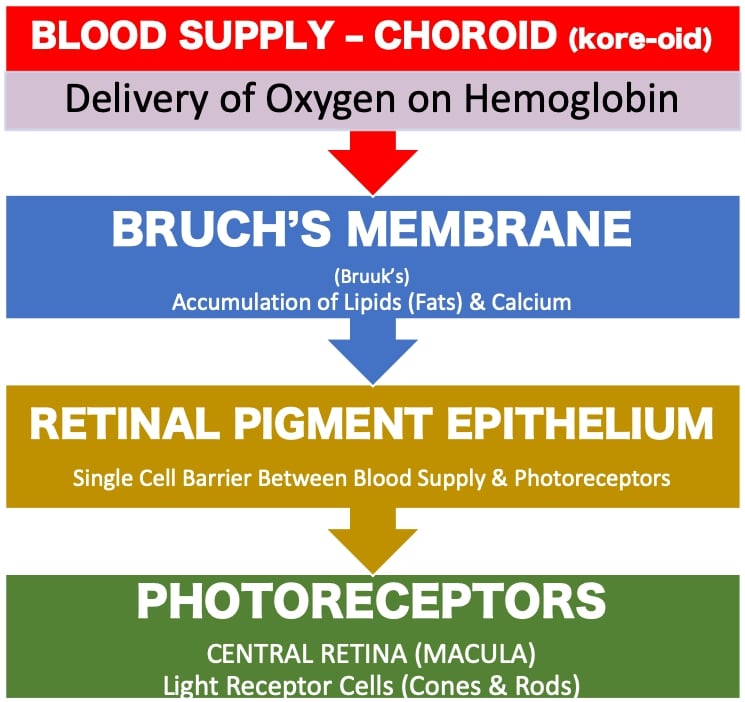
The blood supply layer of the retina (choroid) is separated from the light (photo) receptors by a thin cellophane-like film called Bruch’s (Bruuks’s) membrane and a single layer thick row of cells called the retinal pigment epithelium (RPE). Calcium and fats accumulate in Bruch’s membrane with advancing age. This membrane doubles in thickness from 2.0 microns to 4.7 microns over ten decades.
It has been argued that lipid (fat) accumulation in Bruch’s membrane does impairs delivery of oxygen to the photoreceptors. However, researchers rule out that accumulation of fats in Bruch’s membrane impairs blood flow or oxygen delivery in any significant way.
A thickened Bruch’s membrane can delay oxygen to the photoreceptors. Calcification of Bruch’s membrane can impair oxygenation. A more acute example is a disease called pseudoxanthoma elasticum which is characterized by calcification throughout the body. Calcification is known to starve the photoreceptors of oxygen and induce destructive new blood vessels (aka neovascularization or angiogenesis) in cases of pseudoxanthoma elasticum.
Blood flow through the choroid is said to be the highest of any tissue in the body but oxygen extraction from hemoglobin is one of the lowest of any tissue in the body (less than 1 volume percent of oxygen). This makes a shortage of thiamine/B1 critical in normalizing oxygen delivery to the retina.
Oxygen levels are high in the barrier layer (RPE) because it is in close approximation to the oxygen-rich choroid. But further away from the choroid, oxygen levels decline to near zero at the photoreceptors in the dark. This near-zero oxygen environment must be a defensive mechanism to limit oxidation. But it also increases their vulnerability to oxygen deprivation.
It has also been documented that as a total oxygen-less state develops in tissues (ischemia/hypoxia), molecular transporters of thiamine are increased on hemoglobin, evidence the body is designed and relies upon thiamine naturally for dynamic defense against oxygen-deprivation.
Of interest, thiamin-deficiency can molecularly elevate a protein called hypoxia-inducing factor (HIF-1) and induce destructive new blood vessels without true oxygen deprivation, a condition called pseudo-hypoxia.
Changes in tissues due to true lack of oxygen (hypoxia-ischemia) are identical to those produced by thiamine deficiency. This suggests many cases of wet macular degeneration may be induced by thiamin deficiency alone, without oxygen deprivation. This may also explain why some patients with wet macular degeneration do not respond to anti-growth factor injections.
The so-called early form of macular degeneration, called the dry form, is distinguished from the wet form by leaky blood vessels (micro-hemorrhages) and oxygen deprivation so acute that new blood vessels outcrop and invade the visual center (macula) of the eyes.
There is no argument that wet-form macular degeneration is triggered by frank lack of oxygenation. In an oxygen-less environment, a growth factor (vascular endothelial growth factor or VEGF) activates the outcropping of invasive blood vessels that destroy the visual center (macula) of the eyes. Eye doctors inject anti-VEGF medications periodically (monthly) to prevent permanent loss of vision.
The less invasive dry form of this disease “can only be caused by ischemia” say researchers at Colombia University Medical Center. And certainly the absence of oxygen also triggers the more severe wet macular degeneration as well.
More specifically, researchers note there are dysfunctional small arteries (arterioles) in the blood layer (choroid) are under the control of the autonomic nervous system (not under conscious control by the individual). Bodily functions like heart rate, respiration rate, temperature control, hunger and appetite, waste elimination, and sweating are automatically controlled in the human body.
Autonomic control goes haywire in dry form of macular degeneration. Colombia University Medical School researchers hypothesize their investigation “supports a parasympathetic (autonomic) control of the arterioles as a causative factor in reduced perfusion (passage of blood) of the area surrounding the RPE (retinal pigment epithelium).”
Not noted by these researchers is that thiamine/vitamin B1 is essential for proper control of the autonomic nervous system.
Normally a transient gas called nitric oxide dilates (widens) arteries to maintain blood flow and pressure. Drugs like niacin and Viagra-like drugs that activate nitric oxide would then have application for this disease. But the production of nitric oxide is impaired due to loss of autonomic control, note researchers. Albeit, the lack of nitric oxide gas is also associated with blockage of veins (retinal vein occlusion) as de-oxygenated blood exits the retina.
Dietary nitrates, such as found in sugar beets, may increase nitric oxide and inhibit autonomic (parasympathetic) constriction of arterioles(small arteries) in the retina. Other molecules found in garlic (allicin) and grape wine (resveratrol) activate nitric oxide and improve circulation. But again, lack of thiamine limits the capacity to produce nitric oxide.
Lack of cell energy is given as another reason why insufficient amounts of nitric oxide gas are produced in certain disease states. Given that thiamine boosts cell energy (adeno-triphosphate or ATP levels) within the atomic power plants (mitochondria) of living cells, it is no surprise to learn that thiamine is a critical nutrient to enabling nitric oxide to do its job of dilating (widening) arteries to improve blood circulation and delivery of oxygen.
In further support of the oxygen deprivation origin of macular degeneration, it is well documented that sleep apnea (stop-and-start breathing during sleep) worsens macular degeneration whereas hyperbaric oxygen treatment is efficacious in preserving or improving sight. Furthermore, in more severe oxygen deprivation (total or near-total absence of oxygen), hyperbaric oxygen rescues patients with wet macular degeneration. Untreated sleep apnea hinders the response to anti-growth factor injections into the eyes of macular degeneration patients.
Consistent with the thiamine-deficiency theory of wet-macular degeneration, it has been shown that a shortage of thiamine promotes more of a protein complex called hypoxia inducing factor (HIF1) that then triggers the production of growth factors (VEGF) that then sprout new blood vessels that destroy central vision. Therefore, thiamine supplementation would be strongly indicated to head off wet macular degeneration and needle-injections of anti-growth factors directly into the eyes. However, use of thiamine to prevent wet macular degeneration remains untried.
Low cellular levels of thiamine results in a decline in cellular energy and poor transport of oxygen to tissues, particularly in the retinal pigment epithelial cells that separate the retinal blood supply (choroid) and the photoreceptors. In a state of thiamine deficiency excess lactic acid is produced in tissues throughout the body. Patients with macular degeneration characteristically exhibit low cell energy and elevated lactic acid.
In 2009 vitamin B1 was heralded as a cure for uveitis, an inflammation of pigmented inner lining of the eye. But it is not known if thiamine has come into common practice in eye clinics for this malady, given modern medicine’s reluctance to embrace nutritional medicine.
An explanation of how laser treatment rescues threatened vision centers on the restoration of oxygen supply to a starved retina. It has been noted that if some retinal photoreceptors are destroyed by laser light, then subsequent scars that form at the back of the eyes allow oxygen to diffuse directly to the inner retina via these laser-induced scars rather than being consumed by the energy-making compartments (mitochondria) of the photoreceptors. With adequate oxygenation, then growth factors are inhibited and destructive new blood vessel formation is halted.
Thiamine deficiency and consequent oxygen deprivation is linked to many other maladies.
Chronic obstructive pulmonary disease (COPD) is a serious lung disease. It takes the breath out of COPD sufferers. It is not surprising to learn that dietary intake of thiamine is lower than the Recommended Daily Allowance in over 75% of COPD patients.
Nor is it surprising to learn that the symptoms of an inherited mitochondrial disorder called Leigh Syndrome (maternally inherited) which encompasses night blindness, nerve disorders and abnormally uncoordinated movements called ataxia, are treated with thiamine.
Thiamine in its fat-soluble form (benfotiamine) is literally curing Alzheimer’s disease as evidenced in brain scans. Given that benfotiamine does not pass through the blood/brain barrier, it is obviously working indirectly (autonomic control or by increasing oxygenation before it reaches the brain?).
Dementia, a progressive decline in mental function, is actually called transient ischemic attack (TIA). Loss of autonomic control is at the core of all chronic brain disorders. Thiamine is considered a protective factor for dementia.
Nor should silent ischemia that produces no symptoms of chest pain be overlooked. Some 3 to 4 million Americans experience silent heart disease (angina).
Regardless of the lack of published evidence, any human disease that involves oxygen deprivation should be indicative of need for thiamine.
It is not difficult to understand why patients with macular degeneration may not exhibit signs or symptoms of oxygen deprivation in other organs and tissues. The human eye is particularly vulnerable to shortages of oxygen.
There are 140 million night vision (rod) cells and ~6 million color vision cells (cones) in the retina. Rods can function in remarkably ultra-low oxygen environment. In the dark the 140 million rod cells devour oxygen and virtually surround and overwhelm the far fewer cone cells, resulting in a zone of near-zero oxygen in the macula, the visual center of the eyes. The central retina has very little oxygen reserve capacity.
An interesting environmental factor that exacerbates any oxygen-deprived tissue is arsenic, a heavy metal contaminant found in water supplies and in the widely used glyphosate herbicide, that can mimic a hypoxic effect. Arsenic can set the stage for oxygen deprivation diseases.
Few if any eye physicians would suspect arsenic toxicity in out-of-control wet macular degeneration or diabetic retinopathy. Without knowledge of their cause, many cases of eye disease that don’t respond to conventional treatment will remain unexplained. Given that glyphosate is associated with kidney disease, it is not beyond the realm of possibility that the more vulnerable retina could also be harmed by arsenic toxicity via pseudo-hypoxia. There is some scientific awareness that arsenic is related to macular degeneration.
Beriberi is the name of the disease symptoms that emanates from a frank deficiency of thiamine/vitamin B1. Oxygen deprivation due to poor transport of oxygen in thiamin-deficient individuals could theoretically produce abnormalities simultaneously throughout the body. However, certain organs and tissues are better protected from thiamine deficiency and therefore other organs may exhibit symptoms of thiamine shortage without resulting in the classic and severe symptoms of beriberi – – the overt vitamin deficiency disease, characterized by pain (calves), loose stool, abnormal heart rhythms, heart failure, involuntary eye movement, paralysis, shortness of breath with activity, swelling in lower legs, loss of muscle control, difficulty speaking, and other autonomic system disorders.
Only recently have researchers recognized that the progression of vision loss due to macular degeneration is not as it seems. The conventional way to assess prognosis is to determine the amount of cholesterol-like deposits (oxysterols) called drusen that appear as yellow deposits at the back of the eyes. Now investigators realize drusen block oxygenation of the retina. Impaired oxygen transport is finally being mentioned as the cause of progressive vision loss in old age. This sets the stage for the preventive and therapeutic use of thiamine, but modern medicine will predictably pursue synthetic drugs rather than a simple nutrient like thiamine/vitamin B1
Thiamine/vitamin B1 is provided in food in small amounts (micrograms) as a water-soluble nutrient. The best diets only provide 1.0 to 2.0 milligrams of thiamine. There is only ~30 milligrams of thiamine stored in the body which will last only 18 days if totally deprived of this nutrient. To ensure human populations receive adequate intakes of thiamine, flour is fortified. According to US Department of Agriculture data, 81.6% of the American population consume an adequate amount of thiamine/vitamin B1.
But public health authorities overlook the problem of absorption. Refined sugars, alcohol, refined carbohydrates (bread, polished rice, cereal and pasta, the basis of the Food Pyramid that public health authorities have now abandoned), as well as coffee and tea, block the absorption of thiamine. Chronic use of antacids or diuretics (water pills) and the lack of stomach acid (often due to H. pylori infection) also block or impair vitamin B1 absorption. Tobacco use (nicotine) impairs cellular use of thiamine. Tobacco use is also a risk factor for macular degeneration as is alcohol.
This is why the more soluble vitamin B1, benfotiamine, was developed. Doses of benfotiamine are high (100-140 milligrams) to overcome absorption problems. However the maximum amount of thiamine that can be absorbed by a single oral dose of thiamine hydrochloride ranges from 4.8 to 8.3 milligrams.
Super-soluble benfotiamine is almost six times more biologically available than water-soluble thiamin hydrochloride, the common form used in dietary supplements. Allithiamine, another form of vitamin B1 available as a dietary supplement, unlike benfotiamine is able to traverse the blood/brain barrier and is advantageous. Sulbutiamine is yet another form of vitamin B1 that is commercially available and is touted for its superior ability to enter the brain.
Almost all multivitamins provide economical forms of vitamin B1 in water-soluble form (thiamine mononitrate, thiamine hydrochloride) that convert in the body to the active from of the vitamin, thiamine pyrophosphate.
Regardless of dosage, side effects are generally not reported with thiamine supplements at any dosage. Thiamine can be taken with any drugs.
Currently there is only one multivitamin (formulated by this author) on the market that provides benfotiamine and allithiamine.
Magnesium is an essential co-factor with thiamine. The lack of magnesium may render supplemental thiamine useless.
Blood tests for thiamine are generally not accurate and only reflect recent consumption. Asking your doctor for a B1 test is a waste of money.
Today we now realize much disease emanates from altered gut bacteria. Gut bacteria is now linked with glaucoma and macular degeneration. The desirable family of healthy gut bacteria known as Bacteriodetes requires thiamine. Some gut bacteria actually synthesize their own thiamine. Thiamine was detected in humans whose diets were completely deprived of thiamine, inferring B1 was derived from their gut bacteria! The human body does everything it can to hold on to this essential nutrient. The promotion of healthy gut bacteria may help explain why benfotiamine, which does not cross the blood/brain barrier, reverses Alzheimer’s disease.
It is unlikely macular degeneration patients will bolt from their eye doctors and venture on their own to use thiamine therapy. Only patients for whom eye injections have failed are likely to consider thiamine vitamin B1 therapy out of desperation.
Many macular disease patients are over-reliant on doctors, cannot make independent decisions, are obviously vision impaired and are likely mentally challenged and are only in a financial position to use medications that Medicare pays for. So it is unlikely aged macular degeneration patients will opt for thiamine pills.
Most if not all macular degeneration patients who inquire about thiamine will be confronted by clueless eye doctors who, even if knowledgeable, will act to protect their incomes. Replacing an injectable drug that costs $9,926-$18,900 a yearwith a 15-40-cent/per day vitamin ($55-150/year) that doesn’t require a prescription is not likely to be embraced by modern medicine.
By personal experience, when a resveratrol pill this writer formulated gained attention in the news media for its ability to spare hopeless macular degeneration patients from vision loss when their treatment failed, eye doctors simply said the pill was unproven and that their injected medicines finally kicked in and the resveratrol pill was worthless. This was despite published reports of its effectiveness. So, like resveratrol, a crusade to get patients to take thiamine pills is likely an exercise in frustration. Doctors have their fallback position: where is the double-blind placebo-controlled study? Yes, where is it?
Thiamine/vitamin B1 blocks the most serious physical consequences of diabetes– heart failure (cardiomyopathy), kidney failure (nephropathy), retinal swelling (retinopathy) and numbness and tingling in nerves in the legs and arms (peripheral neuropathy), yet modern medicine shuns thiamine therapy.
Macular degeneration runs along family lines. There is considerable increased risk to develop macular degeneration if older family members have the disease. The lifetime risk for macular degeneration is ~50% for those with family members who have the disease and only 12% for those who don’t, a 400% difference. These at-risk individuals who fear losing their sight to the same disease their grandmother suffered with, are the most likely to practice prevention and consider thiamine/vitamin B1 therapy.
People don’t need a disease to supplement their diet with thiamine/vitamin B1. Life ceases without B1. Given the calorie-rich modern American diet is rich in vitamin B1 blockers (sugars, carbs, alcohol, B1 blocking drugs, antacids, antibiotics, even coffee and tea), Dr. Derrick Lonsdale characterizes this as “high calorie malnutrition.” Intake is adequate, absorption is blocked and the masses suffer.
Given the current set of circumstances in the 21st century, it is difficult to conceive that ANY American child or adult has adequate thiamine nutriture. Proceed without thiamine at your own risk. Don’t forget the accompanying magnesium.
Posted in Vitamins ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105