
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted March 24, 2021: by Bill Sardi
In the war against COVID-19, the most experimental of all vaccines, RNA inoculum in place of pathogenic bacteria or viruses, were introduced first and thrust upon military and healthcare workers, as well as the most vulnerable (elderly, African Americans) who are also the least likely to benefit and most likely to experience severe side effects, turning humanity into one giant global guinea pig lab.
When the race to gain licensure for vaccines by the Food & Drug Administration began, health authorities said they expected four of the first seven vaccines to fail. Confusingly, RNA vaccines are also said to be 95% effective.
Three decades of research efforts to produce an RNA vaccine did not produce a successful track record. But an RNA vaccine would now be successfully developed in just a few weeks, if we are to believe the press releases of the vaccine makers (with information about their stock prices at the bottom).
Since many who read this report have already elected to undergo immunization with an RNA vaccine, be forewarned this report may shake your faith in these vaccines.
The current COVID-19 coronavirus pandemic resulted in renewed attempts to produce an RNA vaccine because this type of vaccine doesn’t introduce a pathogenic virus into a recipient’s body as conventional vaccines do in order to produce protective antibodies. Therefore vaccine-induced infection cannot occur. RNA vaccines send the same genetic signal to produce antibodies within living cells without actually having to infect patients with an attenuated (weakened) virus or viral particle. And RNA vaccines do not include toxic adjuvants like aluminum to provoke an immune response.
Regardless of the advertised effectiveness of these RNA vaccines against COVID-19 coronavirus, there is only a remote chance anyone will benefit from these vaccines. Thousands of people must be vaccinated who don’t have any infection to find a few subjects with active cases of COVID-19 infection, among whom protective antibodies will then be produced.
A phase 3 study of an experimental COVID-19 vaccine is revealing. Among over 43,000 total participants (half given the RNA-vaccine and half an inactive placebo shot, or about 21,000 in each group) only 170 cases (4/10ths of one-percent) of infection were tabulated using the woefully inaccurate PCR swab test that produces >50% false positives, with 162 cases in the placebo group and 8 cases of infection in the vaccine group, for a reported effectiveness of 94%.
The RNA vaccinated subjects experienced broad activation of antibodies and T-cells. Presumably 154 cases of infection would have occurred in the vaccine group out of ~21,000 vaccinated, which is only 7/10ths of one-percent.
The mistaken presumption is that the vaccinated participants will have developed long-term immunity against this dreaded virus as most school children do when they are inoculated against measles, chicken pox, etc. Even if these inoculated individuals weren’t exposed to COVID-19 during a study period, they would be protected against future infection.
However, now investigators report there is no immunity against newly mutated forms of COVID-19 that are now overtaking earlier genetic strains.
A former FDA commissioner has recently warned that experimental vaccines now under evaluation do not protect against COVID-19 coronavirus variants (mutations).
So immunized subjects may be re-infected.
As new genetic strains of COVID-19 take over, immunity may be fleeting and vaccinated individuals would have only developed temporary immunity and transiently benefited from vaccination.
Vaccine makers are declaring their RNA vaccines “safe” before that fact is proven. Among the first 1,893,360 first doses of Pfizer COVID-19 administered, there were 4,393 adverse events (about 2/10ths of one-percent), some life threatening. Those who experienced a serious side effect risked their lives for temporary immunity against a dreaded virus whereas 95-99% of people who acquire this infection get well on their own. The safety reports the public reads about in the news media is smoke and mirrors.
Side effects of RNA vaccines are expected to be latent, months to years after initial inoculation. Some vaccines have been recalled long after gaining FDA approval.
Early experimental RNA vaccines in the 1990s produced a vexing overreactive immune response in animals. Then in 2005 researchers believe they overcame the early recognized problems by replacing one of the components of RNA vaccine (pseudo-uridine in place of uridine) to weaken immune sensitivity which supposedly improves safety. But weakened vaccination is imperfect vaccination.
Imperfect vaccination resulting from “leaky vaccines” wherein a virus escapes immune surveillance is a known problem. Did the investigators in their zeal to develop a less problematic RNA vaccine end up producing a leaky vaccine?
An imperfect vaccine keeps infected subjects alive but still allows transmission via shedding of viruses that could result in the circulation of very virulent viruses in a population. The RNA vaccines may suppress symptoms, but not transmission to others, thus making the vaccinated super-spreaders.
A vaccine that eradicates less virulent viral strains may allow more deadly viral mutations to prevail. This is called the “imperfect vaccine” problem. The substitution of pseudo-uridine in place of uridine in RNA vaccines may have created “imperfect vaccination.” Virologists know this but are tight-lipped.
Obviously, mutations cannot occur if the virally-infected cells are killed. But a so-called leaky vaccine whereby viruses escape immune surveillance and eradication gives more time for viral mutants to form. Under some circumstances vaccination itself may be the key driver that creates a more deadly viral strain. This appears to be what is happening now with RNA vaccines.
These widely touted RNA coronavirus vaccines may be no better than marginally effective seasonal flu shots that frequently do not immunize against the dominant flu virus in circulation during any particular flu season because flu viruses mutate rapidly.
Even though readers will be confronted by (mis)information that COVID-19 is far more prevalent and deadly than the seasonal flu, that conclusion is drawn from use of a rigged PCR blood test and over-categorization of deaths as “caused by COVID-19.”
When blood tests for antibodies were drawn, the infection/fatality rates were about the same for COVID-19 as seasonal influenza. However, mortality rates from variant forms of COVID-19 are not yet known.
It appears the vaccine industry and public health officials want to inoculate vulnerable individuals against each and every variant of COVID-19 rather than create trivalent vaccines like those that include three flu strains-in-one shot.
There is along list of COVID-19 variants. For comparison, influenza viruses mutate so rapidly the three-strain seasonal flu shot often does not include the dominant flu strain in circulation in any given flu season. The current RNA vaccines, as advanced as they may be, may end up chasing yesterday’s, not today’s, coronavirus strain.
Despite face masks, social distancing and hand washing, there is no way to completely prevent exposure and subsequent infection by COVID-19. Many more people are exposed and infected by COVID-19 than the number of laboratory-confirmed cases. COVID-19 is highly infectious but usually produces mild symptoms with as many as 50% being asymptomatic.
Adding to the public’s confusion is that many asymptomatic people submit to PCR testing to see if they are COVID-19 positive when they are falsely positive. What is the difference between an asymptomatic patient and a false positive patient? That goes unexplained.
The PCR test is often set to detect even a miniscule number of viral particles, not enough to cause symptoms and maybe only dead virally-infected cells. These PCR test is commonly misinterpreted as positive. The PCR test is known to produce pseudo-epidemics. Be aware, you may be attempting to prevent or treat an infectious disease that isn’t there. And losing a lot of sleep over it to boot.
In the US, about 30 PCR tests are performed to find one COVID-19 positive case. For comparison, in Australia and New Zealand, ~5000 PCR tests have to be performed to find 1 positive case of COVID-19.
An explanation for this wide difference in infection rates is obvious. US labs skew the results by doubling the count of viral particles 35-40 times. This is why there are so many false-positive PCR tests for COVID-19.
A New York Times study determined about 63 percent of these PCR tests would no longer be judged positive if the cycles were limited to 30. So, before you write your last will and testament because you tested positive, realize if you lived in New Zealand the test may have a different interpretation.
Given that antibodies are not long lasting and may even induce worse outcomes, it is important to develop vaccines whose effectiveness is not solely determined by antibodies.
Viruses are not live. They need to enter living cells and use the genetic machinery of your cells to make copies.
According to Dr. Andrea Branch at the Icahn School of Medicine at Mt. Sinai in New York, the main objective should be to activate T-cells (viral killing cells produced in the thymus gland), not fleeting antibodies.
In a landmark report published in Hepatology Communications (volume 4, No. 12, 2020) Dr. Andrea D. Branch instructs:
“Ideally, at the conclusion of an infection, the body is left with memory T and B cells that are ready to react quickly, preventing infection if re-exposure occurs. The goal of vaccines is to mimic this process and stimulate the production of memory T and B cells.”
T-cells are dependent on the trace mineral zinc. T-cell function is particularly susceptible to zinc deprivation.
The problem with zinc is that it is going to pour rain on the RNA vaccine parade.
Of course, vaccinologists give a thumbs down to mega-dose (220 milligram) zinc for COVID-19 (this report is posted by Google at the top of any online search for “COVID-19 and zinc”). Nor did a 50 mg dose of zinc shorten the course of COVID-19 infection. And justifiably so because such a high dose of zinc simply cleaves more if this trace mineral to its binding protein (metallothionein) which protects against zinc toxicity. Therefore, very little unbound (free) zinc is available.
Dr. Ananda Prasad, the reigning authority on zinc nutrition, suggests no more than 30 milligrams of supplemental zinc as a safe and effective dose so it won’t all be bound up by its carrier protein.
Poorly-trained virologists who often cast a blind eye at nutrition may not realize that zinc is often not bioavailable without accompanying selenium, another trace mineral that facilitates the release of zinc from metallothionein.
Zinc is reported to block the replication of coronaviruses, which is the most effective way of nixing this infectious disease.
Recognize that zinc facilitated T-cell immunity is a “universal vaccine” against any and all viral strains, any virus, any genetic strain.
Even a marginal zinc deficiency can result in a shrunken thymus gland and weakened immunity. Modern medicine totally ignored across-the-board zinc supplementation, especially important for frail elderly individuals and growing children as well as fertile females.
COVID-19 is a highly infectious virus. Wearing face masks, isolation, social distancing, only delay the spread of the disease, they do not prevent disease. I think every person I know has revealed to me they have had a bout of infection in the past year that produced symptoms common to COVID-19. With infection inevitable, the best approach is to block replication of the virus in your body.
If a sterilizing vaccine is employed, transmission to others is completely halted. However, viruses can’t be killed since they aren’t live material, but the cells they reside in can be.
Better for modern medicine to chase down molecules that universally interfere with the replication of every class of viruses than to create a myriad of vaccines that are often off the mark due to viral mutation.
Remdesivir is a widely promoted anti-coronavirus drug that binds to COVID-19 polymerase, the enzyme that facilitates replication of the virus. However, among off-the-shelf molecules that mirror the same protective effect of remdesivir are quercetin, fisetin, resveratrol and green tea.
Once again, these natural molecules are effective against any and all genetic strains of coronavirus.
Resveratrol, known as a red wine molecule, is 98% effective at inhibiting the replication of COVID-19 infected cells in a lab dish. An authoritative report concludes these molecules “represent a valuable therapeutic strategy for the management of COVID-19 infected patients.”
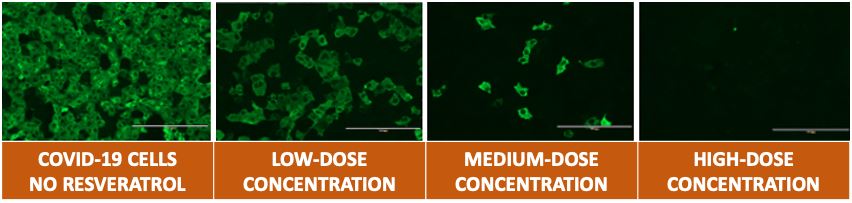
Effects of Resveratrol on COVID-19 replication in living cells by dose concentration in a lab dish.
Source: Phytotherapy Research, Sept. 2020
Allicin, the primary molecule produced when garlic cloves are crushed, blocks the protease enzyme that facilitates replication of coronaviruses. Alkalinized garlic capsules negate the destruction stomach acid has on the enzyme (alliinase) and assuredly facilitates the production of allicin.
Every RNA vaccinated individual needs to prophylactically alter their diet towards lysine (cheese) over arginine (nuts, chocolate) since arginine facilitates replication of the virus and lysine blocks it. For surety, L-lysine supplements should be taken prophylactically and if showing symptoms of infection (coughing, fever, breathlessness, etc.), lysine dietary supplements should be employed. These natural remedies work universally and are not strain specific.
I say to almost every person who has a positive PCR test for COVID-19, you may or may not have experienced COVID-19 infection in the past year because COVID-19 symptoms may be mimicked by a vitamin B1 (thiamine) deficiency induced by over-consumption of alcohol, polyphenols in coffee or tea, and by sugary foods. Alcohol consumption is up 500% in America.
There is strong evidence that increasing sunshine vitamin D blood levels reduce COVID-19 “positivity” (12.5% were COVID-19 positive with less than 20 nanograms/milliliter vitamin D; 8.1% positive with 30-34 ng per milliliter; and 5.9% with vitamin D blood levels of 55+ ng/milliliter), and this protective relationship persists regardless of latitude, race-ethnicity, gender and age.
The data are clear — vitamin D supplements reduce mortality rates for COVID-19 infection, again, any variety or mutation of coronavirus.
The very fact coronavirus infections are seasonal suggests low sunshine vitamin D blood levels are to blame. In winter the rates of heart disease, multiple sclerosis, mental depression (seasonal affective disorder), cancer and of course infection disease, all rise.
Even more convincing, data reveals adequate vitamin D blood levels drop the fatality rate from COVID-19 infection from 21% to just 3%.
Vitamin D adequacy also explains why COVID-19 infected individuals are asymptomatic.
Do we need any more evidence?
No wonder when modern medicine went to determine how much vitamin D is needed it fabricated a “statistical error.” The Recommended Daily Allowance is 600 units, equivalent to 5 minutes of sun/skin exposure. The corrected error is ~8000 units of supplemental vitamin D, equivalent to 30 minutes of midday sun. They now call this: “The Big Vitamin D Mistake.” Nothing like making sure there are enough people with vitamin D-related disease to treat.
What is most feared is months after RNA immunization there is exposure to another one of the seven corona cold viruses. Then the immune system may be triggered against internal organs of vaccinees. In the event of this autoimmune attack, natural molecules that tame down and normalize the human immune response are needed, namely: namely vitamin D, vitamin A, the trace mineral zinc and the red wine molecule resveratrol which sensitizes cells to vitamin D.
Posted in Uncategorized ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105