
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted May 10, 2021: by Bill Sardi
New Gene-Altering Drug Reveals How Drug Companies And Clinicians Use The FDA-Drug Approval Process To Plunder Pools Of Insurance Money While Denying Proven Natural Remedies
The anticipated FDA approval of an injected drug that will lower a risk factor for heart attack which is not addressed by statin cholesterol-lowering drugs has American medicine salivating.
The drug would only need to be injected twice a year. Patients with elevated lipoprotein(a) levels, which is a fatty protein produced in the liver that enters the blood circulation and increases risk for a heart attack, primarily affects 1 in 250 individuals worldwide with a family history. About 60 million Americans have elevated Lp(a) levels. Roughly 1 in 7 heart attacks are associated with high Lp(a) levels, but may not be causal for heart attacks, as you will learn below. Concentrations of Lp(a) vary by 1000-fold between individuals.
Use of this new drug would likely expand to others without a family history but with elevated Lp(a) blood levels, so it could become a bonanza for cardiologists and the drug industry — $1.5 billion sales projected by 2030.
A typical cardiologist may have 3000 active patients. Just think, every Thursday the cardiologist can process 100 patients through his office for injection with this new drug, and @$500 injection fee (not counting the drug itself), bill insurance for $50,000. Treating all 3000 patients would generate $1,500,000 income. The patients will read their blood test and see their Lp(a) levels declined and get a false sense of security.
Researchers in Denmark measure the increased relative risk for a heart attack based upon the Lp(a) level. [Circulation 2008 Jan 15; 117(2):176-84]
| Lp(a) level | Relative risk for heart attack |
|---|---|
| 5-29 mg/dL | 1.1 |
| 30-84 mg/dL | 1.7 |
| 85-119 mg/dL | 2.6 |
| 120+ mg/dL | 3.6 times greater risk |
But don’t be fooled by the above numbers. What goes unexplained is why children can be born with high Lp(a) levels and not experience any increased risk for heart attack, a factor that will be explained below.
The Lp(a)-lowering drug under investigation is Olpasiran (formerly AMG 890) and is a novel small interfering RNA (RNAi) drug intended to lower levels of lipoprotein(a) that is more of a risk for a heart attack than cholesterol. A news report published in the Daily Mail states this new drug genetically “silences” the major cause of heart attacks via correction of a gene defect.
RNAi, is a mechanism present in living cells that inhibits the expression of a specific gene, thereby affecting the production of a specific protein – in this case, lipoprotein(a).
A report on the clinical effectiveness of Olpasiran published in the Nov. 12, 2020 issue of CIRCULATION says there are no approved drugs for elevated Lp(a) levels.
Olpasiran was experimentally used among patients with Lp(a) levels of 70-199 nanomole/liter blood sample in a Phase I human study. Single-dose Olpasiran injections lowered Lp(a) levels by 75-89% more than a month after treatment. The effect lasted more than 6 months for doses of 9 milligrams or higher. But since only around 8 heart attacks occur among 100,000 adults in a year, it is difficult to determine in a small study if an injected drug will actually save lives. The risk reduction is an assumption.
The target stock price of its maker rose to $275 on word of this interim success and projections Olpasiran will generate $1.5 billion in sales by 2030. Olpasiran may be good for a drug company but not for patients. It may only lower a number, not prevent heart attacks. Here is why.
Approximately 20% of the global population (1.4 billion people) have elevated levels of Lp(a) associated with higher cardiovascular risk. Data reveals elevated Lp(a) increases the risk for a heart attack by 20% over a 10-year period in females and 35% in male smokers over age 60 with high blood pressure.
In another recent study, with the assumption of causality, an 80% reduction in Lp(a) would predictably reduce risk of coronary heart disease by 24.4%. But that risk reduction would be over a period of years. Furthermore, that is a relative number, not a hard number, less than a 1% decrease in heart disease in hard numbers. Like all drugs, thousands must take the drug for very few to benefit.
RNAi drugs degrade Lp(a)-producing microRNA inside cells. Delivery of Olpasiran is accomplished by encapsulation in a nanoparticle so it doesn’t degrade before it enters cells. Olpasiran must not activate the immune system which would ignite inflammation. The risk that an RNAi drug would interfere with off-target also genes remains a potential problem.
It is interesting to learn that species of animals that internally produce a natural form of vitamin C (ascorbate) do not exhibit elevated levels of lipoprotein(a), but humans, monkeys, guinea pigs and other species that have incurred a genetic mutation resulted in an inability to synthesize vitamin C, do have variable levels of lipoprotein(a) in their blood serum.
In a legendary experiment, researchers Matthias Rath and Linus Pauling removed vitamin C from the diet of a guinea pig and noted the development of arterial plaque that contained lipoprotein(a). The provision of supplemental vitamin C, at an oral dosage of 40 milligrams per kilogram of body weight, which is equivalent to 2800 mg in a 160-pound adult human, completely abolished arterial plaque formation. It’s like modern medicine simply erased this 20-year-old study.
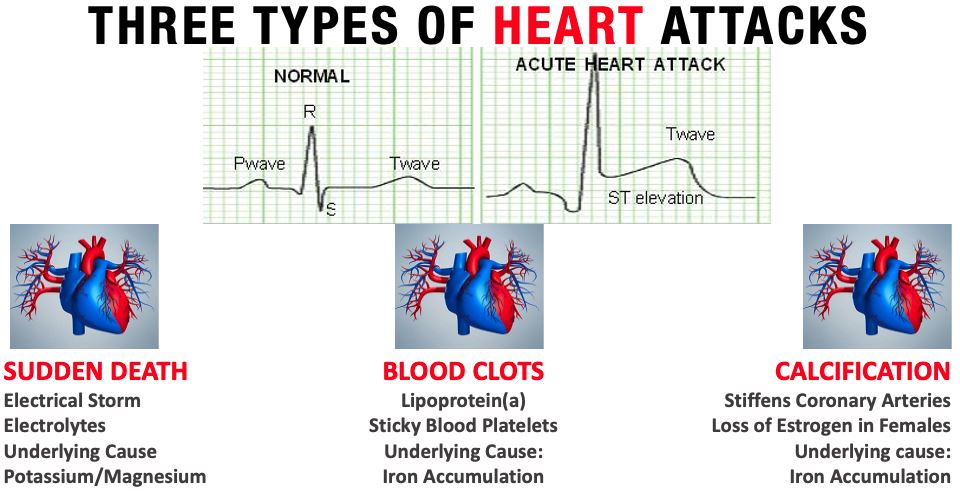
The lack of vitamin C in the diet allows lipoprotein(a) to weaken arterial walls. Lipoprotein(a) is a “sticky bandage” that induces blood clots via attraction of blood platelets that can then impair circulation to the heart and induce a heart attack.
Lipoprotein(a) is perplexing to doctors and patients alike. Lp(a) has been called a “mysterious factor” in heart disease.
The reason for all the confusion surrounding Lp(a) is that cardiologists want to lower a number. It was investigator Matthias Rath who showed that Lp(a) is a substitute for vitamin C within arteries that supply oxygen to the heart. When vitamin C levels are low a lesion or wound in the artery wall develops. Lp(a) is a sticky bandage for that lesion. Lp(a) causes blood platelets stick to the arterial wall. High-dose vitamin C does not lower circulating levels of Lp(a). Vitamin C keeps Lp(a) from being incorporated into artery walls and attracting blood platelets that result in blood clots, regardless of Lp(a) levels. This has been well documented since 1990.
There is no correlation between lipoprotein(a) and other known risk factors for heart disease such as age, sex, blood pressure, body mass index, inflammation (C-reactive protein) and albumin. There is a good reason why. Explanations for this type of heart attack do not include vitamin C.
How did modern medicine get side tracked about the importance of lipoprotein(a) when Drs. Linus Pauling and Matthias Rath conducted ground-breaking experiments in the 1990s that clearly showed Lp(a) replaces ascorbate (vitamin C) in artery walls when vitamin C levels are low, resulting in a weakened arterial wall? It has been known for some time that injury to the internal walls of arteries are milder in areas that have higher levels of ascorbate (vitamin C).
A report published in 1957 in the Canadian Medical Association Journal, thirty-three years prior to the animal study conducted by Linus Pauling and Matthias Rath, clearly demonstrated that arterial plaque can rapidly form in animals without intentionally over-feeding them cholesterol but by depriving them of vitamin C. Early plaque formation could actually be reversed with provision of vitamin C!
Let us not overlook the fact that Dr. Linus Pauling published a book in 1970 entitled Vitamin C And The Common Cold and the intake of vitamin C (largely from dietary supplements) rose 300% and a steep decline in mortality from coronary heart disease was clearly documented. But vitamin C was never adopted into cardiology’s armamentarium and never became public health policy
Adding to the Lp(a) puzzle is that while it is assumed that elevated Lp(a) levels are not favorable for survival, studies reveal high Lp(a) levels are found more frequently among centenarians. Go figure.
Elevated Lp(a) numbers in centenarians may reflect accumulation of iron in body tissues, another fact that is discussed below.
Iron is in short supply during the growing years of life as it is needed to make new red blood cells. Only when childhood growth has ceased does iron begin to accumulate, first in males and later in females when their monthly menstrual flow ceases with the change of life.
Examine these facts.
It is also interesting to note that high blood serum levels of Lp(a) are accompanied by high iron storage (ferritin) levels and low albumin levels (albumin helps to control iron) in cases of severe stroke.
The only certain way to reduce Lp(a) (up to -80%) is to remove Lp(a) outside of the body in a process called apheresis, which is quite expensive and impractical. The unequivocal way to temporarily reduce Lp(a) is by blood filtration (apheresis), which, by the way, also reduces stored iron (ferritin).
It is the accumulation of iron, as measured by the iron storage protein ferritin, that appears to be involved in the reduction of Lp(a). Furthermore, ferritin (iron storage) is also independently associated with arterial calcification. Healthy ferritin levels are 20-90 nanograms.
Iron appears to be a major underlying factor in the reduction of circulating levels of ascorbate (vitamin C) and resultant incorporation of Lp(a) and calcium within artery walls.
Furthermore, modern dietary habits can also help explain, with all of the medical technology available today, why mortal heart attacks still occur. The consumption of refined sugars in sweetened beverages raises circulating levels of Lp(a). High-fructose corn syrup, now added to many foods and beverages, increases the risk for iron overload in the liver, where Lp(a) is synthesized.
| RAISES LP(A) | LOWERS LP(A) | PREVENTS INCORPORATION OF LP(A) INTO WALLS OF BLOOD VESSELS |
|---|---|---|
|
IP6 rice bran (unknown)
|
Vitamin C pills
40 mg per kilogram (2.2 lbs.) body weight or 2800 mg for a 160-lb adult 500 mg/5 times a day
|
It is no secret that the natural decline in estrogen production, beginning around age 54, results in a rise in lipoprotein(a). [Journal American College Cardiology July 2008; Journal American Medical Assn. April 12, 2000] Menopause is when women begin to lose their ability to control iron via monthly blood loss.
Hormone replacement therapy has been documented to reduce lipoprotein(a) levels by 19.9%, 23.0%, 20%, 31%, 28% and 13% in various studies. [Hormone Metabolism Research Sept 2006; Arteriosclerosis Thrombosis Vascular Biology Sept 1997; Arteriosclerosis Thrombosis Feb 1994; Arteriosclerosis Thrombosis Vascular Biology Oct 1996; Obstetrics Gynecology Dec 1996; Journal Clinical Endocrinology Metabolism Nov 1997]. But estrogen replacement may not prevent Lp(a) from inducing blood clots.
Vitamin C is posed as the antidote to heart attacks caused by elevated lipoprotein(a) levels. [Knowledge of Health]
One study shows that men who use supplemental testosterone decrease their lipoprotein(a) level by 37%. [American Journal Cardiology June 1996]
The cut-off-point where Lp(a)-lowering treatment should begin lies somewhere between 30-50 mg/deciliter of blood serum. However, all African Americans would require treatment using this as a measure.
Also there are confounding reports that show (1) elevated Lp(a) does not predict cardiovascular disease among adult-onset (Type 2) diabetes and (2) there is a greater risk for cancer among individuals with Lp(a) below 80 mg/deciliter.
Furthermore, there are other non-prescription medicines and supplements that lower Lp(a) levels. The best known agents that lower Lp(a), aspirin, niacin, L-carnitine, apple pectin, vitamin D, lower Lp(a) by 20-35%.
A person with an Lp(a) level of 200 mg/deciliter taking an anti-Lp(a) agent that reduces Lp(a) to 130 mg/deciliter (-35%) still leaves the patient in the high-risk range.
Bottom line: don’t forget the importance of vitamin C. Researcher Dr. Matthias Rath wrote an entire book about the fact vitamin C-secreting animals don’t get heart attacks, humans do.
Most animals produce vitamin C throughout a 24-hour day. Animals convert blood sugar (glucose) to ascorbate (vitamin C) via an enzyme in the liver (gulonolactone oxidase) as documented by biochemist Irwin Stones in 1979.
The more stress an animal is exposed to, the more sugar that is released into the blood circulation, which then enzymatically results in more vitamin C being endogenously produced. So, humans require more vitamin C when under emotional or physical stress. Essentially, vitamin C is an anti-stress hormone in most other mammals.
The restoration of internal vitamin C secretion in humans would be the ideal. This has only recently been accomplished, and is commercially available, but again, ignored by modern medicine.
©2021 Knowledge of Health, Inc.
Posted in Heart, Uncategorized, Vitamins ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105