
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted March 23, 2018: by Bill Sardi
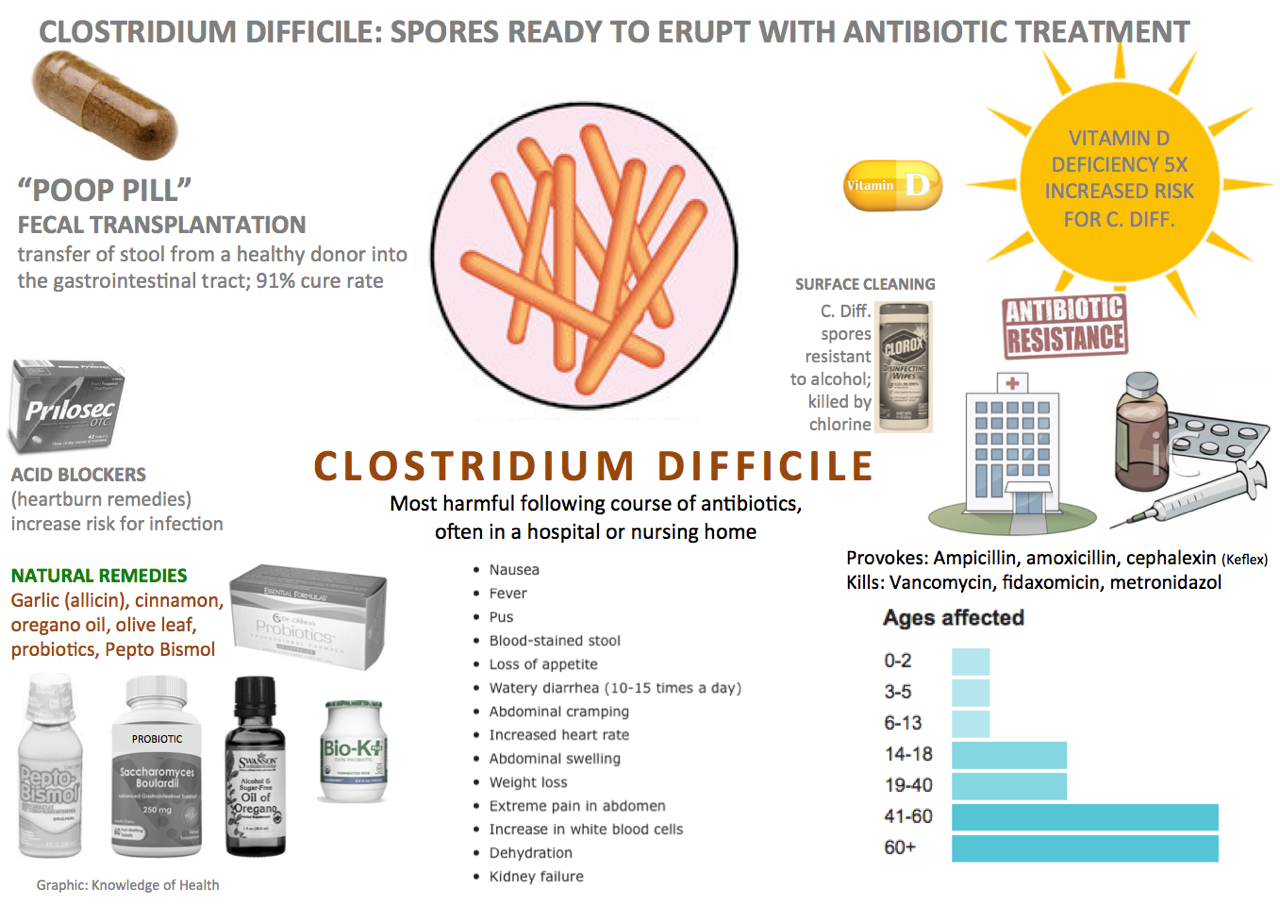
As deadly as Clostridium difficile infection is, just like Count Dracula who was vulnerable to garlic and sunlight, so is this pervasive bacterium.
What modern medicine is unwilling to say is that the digestive tract of every human being harbors a potentially mortal soil organism that is killing off a growing number of Americans. A recent report says: “clostridium difficile infection is not new, but it is posing more problems than ever before.” People aren’t suddenly infected by Clostridium difficile via contact with pets, foods or human-to-human transfer of this bug. They already had it as part of the makeup of 100 trillion organisms that inhabit the human gut (intestines). Healthy digestive tracts resist growth of C. diff. Only an abundance of various families of healthy gut bacteria protects against a raging infection.
This bacterium erupts and produces symptoms after sterilization of the digestive tract by antibiotics when there are no opposing bacteria to keep it in check. With 269.4 million antibiotic prescriptions in the U.S. 2017, that is a lot of opportunity for a potentially lethal germ to produce a long list of agonizing symptoms for a lot of people. C. diff amounts to ~$3 billion of associated expenses.
In particular, three antibiotics, ampicillin, amoxycillin and cephalexin (Keflex) provoke spores to erupt from Clostridium difficile bacteria in the intestines. Antibiotics fidaxomycin and metronidazole are often effective at curing C. diff and Vancomycin, the most effective antibiotic, is usually held as the antibiotic of last resort should all other antibiotics fail. Between 20% and 35% of patients treated with antibiotics will fail initial antibiotic treatment. But antibiotic resistance can occur. Then patients are out of luck.
When all else fails there is transplantation of healthy fecal bacteria transplantation. It is 92% effective at quelling this disease.
C. diff. spores are spread by pets, water sources, root vegetables and soil. One study shows the most common routes of transmission are contact with symptomatic carriers (53%), hospital environment (40%) and non-symptomatic carriers (20%). C. diff carriers with symptoms are 15 times more likely to transmit this germ to others than non-symptomatic carriers. But there is growing concern that non-symptomatic carriers are spreading C. diff outside the hospital.
More often C. diff spores are expelled in human waste and contaminate bathrooms and hospitals and its victims are then re-infected. C. diff spores can remain on surfaces for weeks, even months. Hand washing and use of chlorine (Clorox) are in order to eradicate this germ but may or may not be effective.
You may have heard Clostridium difficile is that life-threatening bacterium that kills elderly nursing home residents. Yes, but it’s creeping into the community because of a quadrangulation of factors: antibiotics, antacid use, vitamin D deficiency and a growing population of older adults whose immune systems aren’t up to par. One study found 53% of healthy human adults tested positive for C. diff in stool samples.
One alarming study shows a third of C. diff cases were not associated with hospital admission, which is a scary finding. The reported mortality rate is 1.0% to 2.5%, amounting to around 14,000 deaths per year.
Why is C. diff becoming a public problem now? It is obvious the gut bacteria of Americans has been unfavorably altered over time.
Health authorities believe the microbiome, the volume and makeup of bacteria in the digestive tract of Americans, has changed over time. Between the 1980s to the present, Americans eating the same amount of food and participating in physical exercise are much heavier. By eating more carbohydrates and fructose-laden processed foods, the makeup of gut bacteria changed. Only 45% of gut bacteria samples from one adult subject were the same 45 years later (1970 and 2016).
The widespread use of high-fructose corn syrup, which is laced into bacon, peanut butter, most prepared meats, baked goods and other processed foods, is of concern because fructose serves as a growth medium for C. diff.
While there is an admitted critical need for non-antibiotic treatments, they are slow to be adopted.
Probiotics, non-pathogenic healthy bacteria, are considered an effective remedy for C. diff. The co-use of probiotics and prebiotics as a preventive measure when antibiotics are prescribed should be routinely practiced by physicians who have been slow to adopt them along with other natural antibiotics like garlic and oregano oil that don’t generate germ resistance.
Among probiotic strains, researchers have found the Bifidobacterium longum probiotic strain is the single most important species of bacteria associated with Clostridium difficile negative tests. Another study identifies Lactobacillus rhamnosus as the most effective probiotic strain (see below).
Clostridium difficile infections are the most common cause of diarrhea associated with the healthcare institutions. One hospital has almost totally abolished C. diff symptoms by use of two capsules of a combination of probiotic strains (Lactobacillus casei and Lactobacillus rhamnosus providing 50 billion healthy bacteria per capsule, commercially sold under the brand name BIO-K), prescribed within 36 hours of antibiotic use. A 2-capsule-a-day regimen (100 billion bacteria) reduced antibiotic-associated diarrhea by 65%, reduced the duration of symptoms (6.4 days shorter) and achieved a 95% reduction in C. diff associated diarrhea cases specifically.
Don’t drop your guard if you believe you have eradicated C. diff after successful treatment. Recurrence rates are high (30-40%). Recurrent C. diff infection is a risk factor for death. C. diff sufferers must be vigilant.
Zinc supplementation favorably alters the gut bacteria and decrease antibiotic resistance to C. diff. Be aware, there are contrary reports warning the public away from high-dose zinc when battling C. diff. However those reports were based upon a study where laboratory animals were given 1000 milligrams of zinc per kilogram (2.2 lbs.) of body weight, or the human equivalent of 70,000 milligrams of zinc (over two thousand 30-mg zinc pills).
Ananda Prasad, the world’s leading authority on zinc nutriture, says up to 45 milligrams of supplemental zinc can be consumed safely without upsetting the zinc/copper balance in the body. Zinc is widely used to quell diarrhea in children. Supplemental zinc reduces infections in the elderly.
Be aware, very little zinc is absorbed orally. The addition of vitamin B6 with zinc (Bio Zinc, Solaray) increases zinc absorption. Accompanying selenium releases zinc from its binding protein to be bioavailable. Organic zinc (selenium attached to an amino acid like selenomethionine or SelenoExcel) is preferred over inorganic selenium (selenite, selenite).
Clostridium difficile should be characterized as the “Count Dracula” of microorganisms because it is quelled by garlic and sunlight. The medical literature shows that the rising rate of C. diff infections and deaths parallel the sun phobia created by the dermatology industry to prevent skin cancer (oddly, deadly melanoma skin cancer often emanates in skin exposed to the sun).
Hospitalized elderly patients with low vitamin D blood levels are almost 5 times more likely to develop C. diff-related diarrhea. (They ought to be adding vitamin D to anti-diarrhea preparations.) This means every hospitalized patient should be screened for vitamin D levels upon admission.
Hospital infectious disease officers must know that C. diff is seasonal, occurring more often in early spring after winter when people spend more time indoors and when the earth tilts away from the sun in the northern hemisphere during winter. Vitamin D is produced naturally in the skin by mid-day sun exposure. Hospitalized patients with blood levels of vitamin D below 10 nanograms/milliliter of blood serum (1000 nanograms per deciliter) were found to be 4.96 times at greater risk for C. diff infection and diarrhea.
The Vitamin D Council suggests up to 6000 units of vitamin D to achieve optimal blood levels.
Here is the C. diff mortality rate experienced by hospitalized patients with recurrent infection according to their blood level of vitamin D:
| Vitamin DBlood level (ng/milliliter) | Mortality |
|---|---|
| Severely deficient: less than 10 ng/mL | 1 in 40 (5.0%) |
| Deficient 10.0-19.9 ng/mL | 1 in 93 (1%) |
| Pre-deficient 20.0-29.9 ng/mL | 2 in 74 (3.1%) |
| Control group Over 30 ng/mL | 2 in 74 (2.7%) |
* All of the above patients should have been considered vitamin D deficient since optimal levels = 40-60+ ng/mL
Hospital rooms are void of sunlight, which is the primary source for vitamin D in the body.
Of acute interest is the fact C. diff spores require calcium to germinate (become metabolically active) and poor calcium absorption due to low vitamin D levels may explain why C. diff often seems to be unconquerable. Calcium supplements for a short time may quell recurrence. C. diff infected individuals may do more to deactivate the spores via calcium and vitamin D intake than be attempting to cleanse their environment. After all, C. diff is everywhere.
While untested, Pepto bismol + water passed through a cloth for filtration will create soluble bismuth that has activity against C. diff and prevents this bacterium from sticking to the wall of the intestines.
Antacids widely employed to relieve heartburn symptoms are particularly troublesome as they negate stomach (hydrochloric) acid that kills off incoming C. diff in consumed vegetables that are grown in the ground (C. diff being a common soil organism.)
Antacids (Nexium, Prevacid, Prilosec) are widely promoted for heartburn but when they provoke a C. diff eruption they can be life threatening. Warnings should be added to antacid labels. One hospital instituted a program to reduce antacid use and reports a 20% reduction in C. diff infection.
C. diff infection rates also rise with use of antihistamines as histamine is required for stomach acid secretion.
Of interest is the role iron plays in C. diff infection. Up to 45% of infants test positive for C. diff. but they rarely develop into symptomatic disease. C. diff and other bacteria require upon iron for growth. Since infants grow rapidly and are chronically anemic as their bone marrow produces millions of new red blood cells per second (iron being required to produce hemoglobin, the red pigment of blood cells), this becomes a mechanism that protects infants from infection of any kind. Full-grown males and non-menstruating females become iron overloaded and are therefore more prone to symptomatic infection. Supplemental lactoferrin, an iron-binding molecule, is posed to inhibit the growth of C. diff.
The age-related decline in stomach acid secretion or the chronic use of antacids, the absorption of vitamin B12 from foods and supplements may not be adequate. Pernicious anemia may result with accompanying symptoms of fatigue, unexplained cough, short-term memory loss, burning feet and unexplained coughs and backaches. A shortage of B12 via lack of stomach acid is associated with but not a cause of C. difficile.
When prescribed antibiotics of any kind, think C. diff. Probiotics (Bio-K), garlic (Garlinex), oregano oil, vitamin D, zinc, calcium, are in order. Some people given antibiotics don’t experience C. diff symptoms till months later. So vigilance is necessary, especially if over age 60.
Posted in Dietary Supplements ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105