
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted May 18, 2020: by Bill Sardi
An estimated 1.4 million more deaths are predicted worldwide from another infectious disease caused by the lockdown and quarantine over the COVID-19 coronavirus fiasco. Yes, that is the alarming increased mortality estimate being issued by STOP TB PARTNERSHIP.
Bottom line, the lockdown and quarantine are going to cause far more deaths from another infectious lung disease than COVID-19.
The worldwide COVID-19 lockdown is disrupting access to care for 1.8 billion people on the planet who have tuberculosis. Some 10 million TB sufferers worldwide fall ill and convert to the active infectious form of TB each year, and 1.5 million die, numbers that far exceed those of COVID-19 coronavirus infections and deaths. But unexplainably, no lockdown and quarantine called by health authorities for a more deadly TB epidemic.
There are ~14 million Americans, the majority who are foreign born, who have TB and another 9000 cases detected annually. Unexpectedly in 2019 TB cases in the U.S. were the lowest ever reported. Around 80% of U.S. TB cases are reactivations from prior latent (dormant) TB. This means the U.S. has a huge population of dormant TB patients that could erupt into active infectious TB at any time, particularly after a very cold winter when sunshine vitamin D levels are low. TB has the same seasonal onset as cold and flu viruses and its prevalence is high among the same high-risk groups – – blacks/African Americans, nursing home patients.
Now, unable to get to doctors and necessary antibiotics, and their immune systems crashing due to the lack of sunshine vitamin D, and possibly living in closer quarters with family members who have latent (dormant) TB, an additional 1,367,300 million TB deaths are expected over the next 5 years.
For every month of the lockdown it is estimated there will be 608,000 more TB cases and 126,100 additional deaths.
|
ESTIMATED GLOBAL IMPACT OF EXCESS TB CASES & DEATHS AS A RESULT OF COVID-19 LOCKDOWN Source: STOP TB PARTNERSHIP |
|||
| Excess Cases 2020-2025 | Excess deaths 2020-2025 | ||
|
2-month lockdown + 2-month recovery |
3-month lockdown + 10-month recovery |
2-month lockdown + 2-month recovery |
3-month lockdown + 10-month recovery |
|
1,826,400 |
6,331,100 |
342,500 |
1,367,300 |
The misdirection in the midst of this live COVID-19 coronavirus epidemic is that 100 vaccines are under development for an infectious disease that is only 120 days old when TB has been around for thousands of years with no vaccine.
Lucica Ditiu, director of the STOP TB Partnership says she is sickened by research that now predicts millions more people are now expected to contract the disease (TB) as a result of the COVID-19 restrictions.
Progress has been made in TB eradication in recent years, but now those infection and death numbers have rolled back to 2013 numbers. According to a newly released report, 6.3 million additional cases of tuberculosis are predicted to occur due to the premature COVID-19 lockdown and quarantine over the next five years. These excess TB cases are predicted to result in ~1.4 million more TB deaths over the next 5 years! (That is in addition to the 1.3 million that typically die of TB annually.)
The predictive study was based upon a 3-month lockdown and 10-months to restore TB care services. California has just extended their lockdown an additional 3 months beyond the initial 3-month lockdown. So, the numbers of TB cases and deaths will rise above these projections.
Currently, TB patients, who are required to report to a TB clinic to monitor their required antibiotic regimen, are in lockdown.
The World Health Organization now says coronavirus is “going to be with us for a long time.” They are whispering about a 3-year lockdown.
Nowhere can anyone find current TB death numbers, likely because they are being misclassified as COVID-19 coronavirus-induced deaths. It is also worth noting that the three hot-spots geographically for COVID-19-related deaths in the world, Wuhan, China; Modena, Italy and New York City, were fighting outbreaks of tuberculosis before the COVID-19 outbreak drew attention because it was allegedly a new mutation of coronavirus that left the entire world population without protective antibodies.
Tuberculosis generally affects younger adults age 18-44 whereas COVID-19 deaths are concentrated in the very old, particularly adults over age 80. It should also be recognized that various vaccines have been under development and tested for SARS coronavirus (inactivated and live-attenuated virus, DNA-based vaccines, recombinant proteins, virus-like particles) for 8 years now, but none have gained final approval.
Microbiologists say the primary clinical difference between COVID-19 coronavirus and tuberculosis is that TB has a slow onset (often many years) whereas COVID-19 erupts within a few days following infection. But frankly, most COVID-19 cases are asymptomatic and those infected are unaware the infection came and went. Only now are investigators becoming aware that co-infection could lead to missing many cases of TB. Or maybe many cases of COVID-19 are solely TB.
Let’s not forget that the Spanish flu of 1918 that reportedly killed 50 million was more recently found to have been caused by tuberculosis by University of California demographers who claim the co-infection of TB plus influenza (H1N1) likely promoted the progression and severity of the pandemic. Thus, two pandemics, viral and tubercular, may now be colliding.
Little is said about the difficulty distinguishing COVID-10 coronavirus from tuberculosis.
This wouldn’t be the first time the same CDC virologists (Fauci, Birx and Redfield) confused TB for a virus. They did it with AIDS says disease investigator Lawrence Broxmeyer MD.
He notes that TB kept cropping up time and again in AIDS patients as the predominant infection leading to death. From the onset, notes Broxmeyer, veterinarian Max Myron Essex, the first scientist to propose HIV testing, knew that TB produces false positive testing for HIV in almost 70% of cases. This caused Essex and his protégé Oscar Kashala to warn that tests for HIV “should be interpreted with caution when screening individuals with tuberculosis or other mycobacterial species.” Other researchers have also found false-positive HIV tests among patients with leprosy who also had TB.
Thermo-Fischer, a $25 billion maker of diagnostic kits for COVID-19 coronavirus, includes Mycobacterium tuberculosis in its list of possible infectious agents that could cross-react in their RT-PCR test for COVID-19, but refuse to release the actual data used to determine this, says Dr. Broxmeyer.
So, is the whole world being misled into thinking deaths are being caused by COVID-19 when mortal outcomes are primarily generated by TB or TB+ COVID-19? And will these hidden TB deaths be used prolong the worldwide lockdown indefinitely and result in futile attempts to develop a vaccine?
The experts claim the reason why 2 million COVID-19 related deaths have not been recorded in the U.S. is because of the lockdown measures. But even if true, what if the consequences of the lockdown are far more destructive and lethal medically than the virus?
The false idea millions will die due to the coronavirus has already been exposed as a mathematical lie. The Bill Gates-funded professor at Imperial College in London, whose 13-year old software predicted millions of COVID-19 related deaths and was used to justify a worldwide lockdown, has been roundly dismissed by other epidemiologists. The coronavirus mastermind at Imperial College has resigned over his own disregard for lockdown measures. The Imperial College death predictions were never verified. Independent evaluators brand those death numbers as “unreliable.” But the death numbers keep being reported on TV.
You may read false reports the COVID-19 coronavirus is causing more deaths than the normal strains of influenza viruses that are in circulation in winter months. But the Centers for Disease Control has been misleading Americans for years that, on average, 36,000 American die of the flu each year. The complicit news media (fake news reporters bought off by big business) haven’t been fact checking the federal government. So how can the public trust the death numbers being distributed by the CDC for COVID-19?
The American Lung Association publishes the true influenza death numbers, as low as 257, 727, and 411 in a year. The CDC combines flu deaths with pneumonia deaths to come up with those numbers in an effort to scare Americans into getting flu shots. The CDC has become the handmaiden of the vaccine makers.
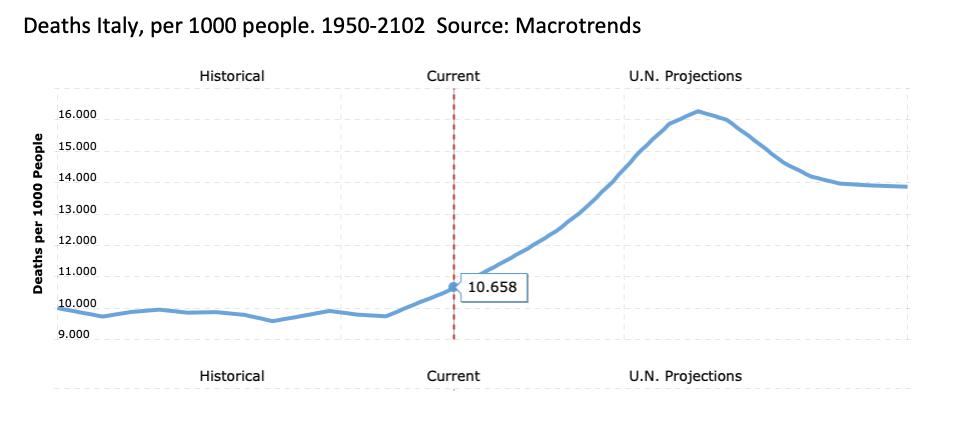
The following chart reveals how the CDC and other scaremongers have maligned mortality numbers to frighten the masses into a contrived lockdown and quarantine. COVID-19 related deaths in Italy have been widely reported. Most of these deaths are among the very old. Examine the graphic below. It shows the number of deaths in Italy (per 1000 people) is already on a steep upwards trajectory because of the large numbers of older Italians age 80 and up, not because of COVID-19. (Graphic Macrotrends)
The COVID-19 mortality numbers are flawed if for no other reason than proof of causality has yet to be confirmed.
In South Africa, there have been 264 COVID-19-related deaths reported (May 18, 2020). But last year there were 63,000 deaths from tuberculosis in a population of 59 million people. The COVID-19 death rate is 0.00000366 or 3 in a million in South Africa. Yet they have been forced into a lockdown with the rest of the world.
Why are microbiologists, public health officials, and the news media, ignoring an ongoing greater epidemic that is already killing millions? Why is the order to lockdown and quarantine issued for a far less deadly coronavirus infection?
Infectious disease experts appear to be leading the world to a literal dead end.
Posted in Coronavirus ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105