
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted September 1, 2021: by Bill Sardi
A heart-breaking MSN news report takes us inside the Children’s Hospital New Orleans to learn that a growing number of kids who are short of breath and for whom there are no emergency-use vaccines, are suffering incessantly. It’s not just COVID-19 lung infections, but potentially life-threating respiratory syncytial virus that can cause some of the same symptoms, says the news report. Parents sleep chairs by their child’s hospital bed in fear they are on the edge of death.
The MSN report goes on to state: “children are struggling to get enough oxygen… some children were suffering more because of underlying health problems, but other severe cases at the hospital had little explanation. A doctor there says: “this is kind of uncharted territory.” If doctors don’t know, then who does?
CNBC reports of a woman who is chronically nauseated and sleepless, 27-year-old runner who is now physically incapacitated. She can’t catch her breath. “I think I’m going to die,” she says. “I was pretty much dismissed by every doctor,” she says. “Just ride it out,” doctors advised her. “They are saying it is COVID, but they also saying they don’t know what to do.” Another patient reports he has no appetite; his symptoms go unexplained also.
The problems are being blamed on widespread vaccine refusal that is spreading COVID. But many of these cases and symptoms are occurring after vaccination.
Normally humans breathe unconsciously. The rate of breathing is controlled by the autonomic nervous system. Healthy people don’t have to think about breathing. It is automatically controlled by blood/oxygen levels.
A University of Nebraska health bulletin states: “Medically speaking, shortness of breath means a patient has to actually think about breathing.”
Shortness of breath, which can occur when someone is anemic (not enough red blood cells to transport oxygen to tissues due to iron deficiency), which is usually resolved by use of iron pills, is not the type of breathing problem that occurs in Covid-19. Young women, anemic due to menstrual blood losses, often experience this form of breathlessness when climbing stairs.
Nor is it the problem of breathing out (exhaling, wheezing) that asthmatics experience.
Nor is COVID-19 lung infection explained by what is called the “cytokine (si-toe-keen) storm.”
The marker for lung inflammation (interleukin-6) is within the normal range in most cases of COVID-19. Respiratory failure in COVID-19 cases is not driven by inflammation per se.
At a “cytokine summit,” held almost a year after COVID-19 was declared a pandemic, researchers noted “disappointing results thus far of IL-6 blockade in numerous randomized clinical trials, several of which have been halted due to futility.”
Doctors call the COVID-19 type of breathing problem “happy hypoxia.” Patients with low blood oxygen levels have no consciousness of oxygen deprivation or what is medically called dyspnea (“air hunger” says the Gale Encyclopedia of Medicine).
This type of breathing problem typically sets in 4-8 days after symptomatic illness begins say Mayo Clinic doctors. Because the blood is not circulating enough oxygen, the heart rate increases to the point where it is racing to keep up with demand for air – a condition called tachycardia.
A physician with 30 years of emergency room experience says he has watched patients come into the ER with COVID-19 and have blood oxygen levels as low as 50%, so low they should have been incoherent, even unconscious. Yet they are completely alert. Normal blood oxygen saturation is between 85-100%, and below 90% is considered abnormal.
Physicians refer to a long list of 25 reasons why the autonomic nervous system is not functioning properly in cases of COVID-19. The lack of thiamine, vitamin B1, is one of them. Intravenous thiamine/B1 therapy increases oxygen consumption. But entire explanations of how to treat long-term autonomic dysfunction in COVID-19 cases, including shortness of breath, don’t even mention vitamin B1, which is not used till the patient is in the intensive care unit. Modern medicine casts a blind eye towards vitamin therapy. It is not mentioned in report after report.
If there is no cytokine storm in the lungs of COVID-19 patients, maybe this is the much-talked-about symptomless (asymptomatic) COVID-19. An estimated 6-41% of COVID-19 patients “may be infected” but have no symptoms. But is there really an infection, or just a false-positive test? Or maybe the infection is not causal and just a by-stander.
Lack of oxygenation can happen when sacs in the lungs are coated with fluid, blocking oxygen exchange. This type of pneumonia can occur secondarily to sedentary patients who don’t exercise and expand their lungs. People taking sedatives (Valium, Ativan, Xanax, Klonopin and Restoril) may not expand their lungs and increase their risk for pneumonia. Anticholinergic drugs (anti-psychotic drugs, antihistamines, antidepressants, anti-Parkinson drugs) increase risk for pneumonia. When these drug-taking patients develop COVID, their risk for pneumonia is further heightened.
Pediatric doctors Mark W. Kline and Stephen W. Hales point their finger at the Delta variant, citing only 37% of the new COVID-19 cases are fully vaccinated. They go on to mistakenly say: “This is largely a pandemic of the unvaccinated… Children under the age of 12 are not yet eligible for vaccination, and the rate of vaccination among adolescents 12 or older is just 12%, but there is so much adults could do to insulate and protect children from this pandemic, just by getting vaccinated. We are not powerless against the delta variant. Vaccination ultimately will rescue us from future surges caused by new variants.”
But this is not borne out by the evidence either. Doctors keep beating their vaccine drum. The children are still suffocating. Vaccines that address new variants will be too late to save many.
Data from Europe reveals 9-months post-COVID infection many patients still experienced symptoms regardless of natural immunity. Patients with persistent symptoms report continued loss of smell (74%), fatigue (53%), loss of taste (31%) and shortness of breath (31%).
The Many Symptoms of Beri Beri (Thiamine B1 Deficiency)Common Among COVID-19 Coronavirus Patients |
|||
|---|---|---|---|
| Loss of smell and taste | Tingling (feet & hands) | Insomnia, oversleeping | Constipation |
| Breathlessness (sailor’s astma) | Involuntary eye movement (nystagmus) | Ataxia (walk like a drunk) | Small intestine bacterial overgrowth |
| Profound weakness | Pain (fibromyalgia?) | Rapid heart rate | Hair loss |
| Cough, hoarness | Memory loss, amnesia | Difficulty speaking | Abdominal pain; hiccups |
| Diarrhea | Confusion, delirium | Swollen lower legs | Distended abdomen |
| Nausea, vomiting | Double vision | Tiny blood clots | Horizontal ridges / nails |
| Loss of hunger (anorexia) | Weight loss / muscle loss | Skin rash | Ear ringing (tinnitus) |
| Fever (from hypothalamus) | Eyelid droop, eyelid twitch | Seizures | Loss of tendon reflexes |
| Heart failure | Kidney failure | Numb feet | Hallucinations / delusion |
| Confabulations | Irritability | Low blood pressure | Celiac nerve pain |
| Learning impairment | Brain shrinkage | Loss of bladder control | Sudden infant death |
| Leaky gut | Slow bile release/liver | Tender calves (legs) | Hypoglycemia |
| Sweating | Hand tremor (Parkinson’s) | Difficulty swallowing | Body stiffness |
| ©Knowledge of Health, Inc. | |||
More specifically, the breathing problem COVID patients experience is called silent hypoxia, which is defined as “a condition where an individual has alarmingly lower oxygen saturation level than anticipated (~ 50–80% saturation, while the anticipated saturation level is 95% or higher). However, the individual does not experience any breathing difficulty.” Normally, an increased respiratory rate is seen in normal hypoxic patients, but this is not typically found in patients with silent hypoxia.
Silent hypoxia (shortage of oxygen) is not uncommon. Several reports revealed that the prevalence of silent hypoxia in COVID-19 patients ranges from 20 to 40%.
Here is what is known that is not being practiced:
Changes in tissues due to true lack of oxygen (hypoxia-ischemia) are identical to those produced by thiamine vitamin B1 deficiency.
It has also been documented that as a total oxygen-less state develops in tissues (ischemia/hypoxia), molecular transporters of thiamine/B1 are increased on hemoglobin, evidence the body is designed and relies upon thiamine naturally for dynamic defense against oxygen-deprivation.
Thiamine-B1 deficiency can molecularly elevate a protein called hypoxia-inducing factor (HIF-1) without true oxygen deprivation, a condition called pseudo-hypoxia.
Bodily functions like heart rate, respiration rate, temperature control, hunger and appetite, waste elimination, and sweating are automatically controlled in the human body by thiamine. These are typical symptoms of COVID-19 patinets. Thiamine/vitamin B1 is essential for proper control of the autonomic nervous system.
Given that thiamine/B1 boosts cell energy (adeno-triphosphate or ATP levels) within the atomic power plants (mitochondria) of living cells, it is no surprise to learn that thiamine is a critical nutrient to enabling nitric oxide (NO), a transient gas produced in arteries, from doing its job of dilating (widening) arteries to improve blood circulation and deliver of oxygen.
Low cellular levels of thiamine results in a decline in cellular energy and poor transport of oxygen to tissues.
Frank thiamine deficiency is called beriberi. Literally organs and tissues may exhibit symptoms of thiamine shortage without resulting in the classic and severe symptoms of beriberi – – the overt vitamin deficiency disease, which is characterized by pain (calves), loose stool, abnormal heart rhythms, heart failure, involuntary eye movement, paralysis, swelling in lower legs, loss of muscle control, difficulty speaking, and other autonomic system disorders.
Thiamine/vitamin B1 is provided in food in small amounts (micrograms) as a water-soluble nutrient. The best diets only provide 1.0 to 2.0 milligrams of thiamine. There is only ~30 milligrams of thiamine stored in the body which will last only 18 days if totally deprived of this nutrient.
To ensure human populations receive adequate intakes of thiamine, flour is fortified. According to US Department of Agriculture data, 81.6% of the American population consume an adequate amount of thiamine/vitamin B1. Most physicians think beriberi is a forgotten disease and can’t recall ever having diagnosed a case.
But public health authorities overlook the problem of malabsorption and reduced transport of vitamin B1. Refined sugars, alcohol, refined carbohydrates (bread, polished rice, cereal and pasta, the basis of the Food Pyramid that public health authorities have now abandoned), as well as molecules in coffee and tea, block the absorption of thiamine. Or chronic use of antacids or diuretics (water pills) and the lack of stomach acid (often due to H. pylori infection) also block or impair vitamin B1 absorption. Tobacco use (nicotine) impairs cellular use of thiamine.
Magnesium is an essential co-factor with thiamine. The lack of magnesium may render supplemental thiamine useless.
The desirable family of healthy gut bacteria known as Bacteriodetes requires thiamine. Some gut bacteria actually synthesize their own thiamine. Thiamine was detected in humans whose diets were completely deprived of thiamine, inferring B1 was derived from their gut bacteria!
Doctors are telling COVID-19 patients with chronic long-term shortness of breath they are simply filled with anxiety and their problems are in their mind. They are advising some of their anxious patients to see a psychiatrist. But a deficiency of thiamine/B1 induces anxiety and vitamin B1 supplementation resolves the problem along with crippling fatigue, headaches, and fevers!
Modern medicine is lost in the woods and is over-committed to vaccination, to the detriment of many people’s health. The answer to this perplexing problem is to obtain a pulse oximeter and measure your own blood/oxygen levels at home. Oximeters cost as little as $30. Oximetry is not reliable at blood-oxygen saturation levels below 80 percent. But pulse oximeters are accurate (within 2% of real values) when blood saturation levels are greater than >90%.
The American Thoracic Society says “most people need an oxygen saturation level of at least 89% to keep their cells healthy”. Some COVID-19 patients have blood/oxygen levels of 80%, 70% or even as low as 50% without shortness of breath!!
Normal oxygen saturation for most people is 94-100% but ER doctors report that a “vast majority” of COVID-19 patients seen at the hospital have “remarkably low oxygen saturations.”
Individuals with early breathing difficulty can take a six-minute walking test. Exercise may induce the problem and provide early detection. After walking for six minutes, a significant decline in oxygen saturation is indicative of silent hypoxia. Oxygen saturation levels below 90% are considered abnormal. A 4% decline is troublesome.
Don’t get too anxious over the test. About 81% of COVID-19 patients have uncomplicated or mild illness and only about 14% will develop severe illness with blood/oxygen levels below 93% and require oxygen therapy.
The window of opportunity is on the fourth to fifth day of illness before the onset of breathing symptoms. Brisk walking back and forth in a straight 100-foot hallway for six minutes (1400 and 1847 feet) will do. Use the oximeter before and after exercise to measure any decline in blood/oxygen levels.
It is imperative that vulnerable patients get ahead of this disease, which may not have a viral origin but rather a nutrient deficiency that acts like a viral infection. In the hospital, a single intravenous dose of thiamine/B1 increases oxygen delivery and consumption.
At home, ill individuals can take preferred fat-soluble forms of vitamin B1 sold at health shops, such as benfotiamine and allithiamine, the latter which passes through the blood-brain barrier. Take as directed on bottle labels.
Don’t attempt to play doctor at home if you have very low blood/oxygen levels. Your red blood cells may begin to stack on top of each other and form clots once this occurs. In the hospital, a D-dimer test will confirm recent over-clotting. COVID-19 survivors have a ten-times lower D-dimer level than non-survivors. Healthy individuals have D-dimer levels less than 0.5 micrograms/milliliter of blood. Anti-clotting medicines may be needed.
Interestingly, thiamine is not known as a blood thinner but the provision of thiamine reduced clotting risk by 81% in one study. In lieu of blood thinning drugs, until you can get to a doctor, the red wine molecule resveratrol should rapidly resolve the clotting problem (see data in chart below).
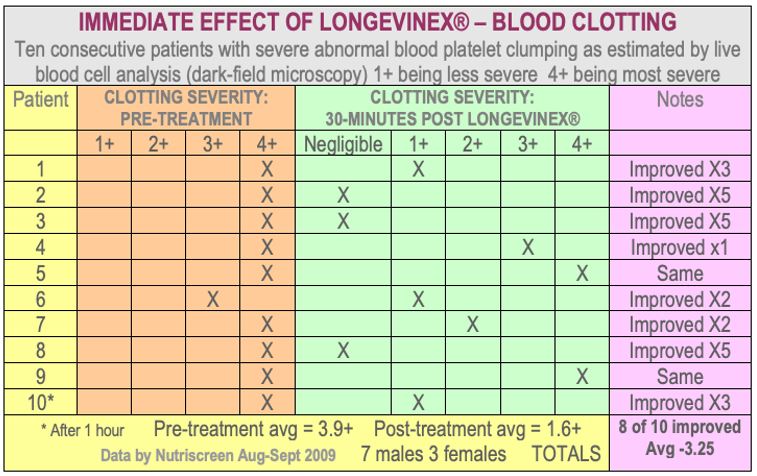
The common blood thinner coumadin (Warfarin) take 30 days to kick in. So, doctors often initially prescribe fast-acting heparin, but in COVID-19 cases clinicians fear a problem called thrombocytopenia (low blood platelet count) with that drug. Already one of the newer blood thinning drugs has flopped for use in non-hospitalized COVID-19 patients. Mild cases of COVID do not require blood thinners at home. But when an oximeter reveals a blood/oxygen level below 90%, the blood clotting risk becomes real. In 2009 a commercially available resveratrol capsule was tested among ten patients with 3+ to 4+ clotting. Eight of ten patients improved within 30 minutes. See chart above.
Enzymes like the pineapple enzyme bromelain or long-acting nattokinase from soy cheese, available at health shops, will also break up both sticky blood platelet and fibrin clots. Nattokinase is a longer-acting enzyme that is also widely available (works for up to 8-12 hours) and is superior in some ways to anti-clotting drugs.
Fish oil and garlic just break up sticky blood platelets but not fibrin clots.
Recognize that thiamine/B1 deficiency, known as beriberi, comes in two forms: so-called dry beriberi which is the neurologic form and wet beriberi where the heart fails and fluid accumulates around the heart and lower legs and there can be catastrophic collapse of the circulatory system. You now may know more than most doctors about the origins of respiratory failure with COVID-19.
Posted in Coronavirus ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105