
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted October 20, 2017: by Bill Sardi
The origin of dyslexia, the neurobiologically-rooted learning disorder that impairs reading words and letters (word blindness) but does not affect general intelligence, is no longer a mystery. As background information, dyslexia is said to affect 5-10% of the population. Some 70-80% of people with poor reading skills are likely dyslexic.
News headlines today herald a breakthrough in the understanding of the biological roots of this disorder. Most scientific investigations into the origins of dyslexia have been focused on the brain. The discovery announced today has to do with eye dominance.
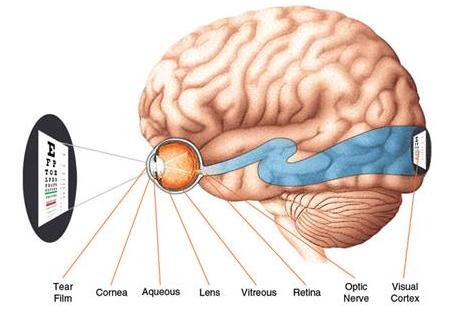
Normally the dominant eye develops a circular cell arrangement in the retina, the light-sensitive film at the back of the eyes that sends signals to the brain via the optic nerve. Researchers discovered both eyes of dyslexics develop this circular cell pattern thus pitting one eye against the other for dominance. This can result in a dyslexic individual seeing a “b” as a “d,” for example.
It is also common for dyslexics to have problems determining which is their dominant hand for writing.

Click On Graphic To View Video On How To Find Your Dominant Eye
One expert said: “What is missing is any suggestion why these differences emerge.”
Well, there is more to be learned than what researchers aired in news reports today.
t appears that dyslexia develops early in the postnatal period. A few weeks after birth a decline in zinc levels occurs in the visual cortex of the brain in animals. The decline in zinc correlates with after the eyes opens, which suggests sensory activation (light) drives the zinc deficiency.
Animal lab researchers report: “the critical period for ocular dominance… roughly coincides with the period of major decline in zinc staining in (the visual cortex) and continues until the end of the second postnatal month.”
Animal eye studies also reveal the electrical circuits in the visual cortex of the brain “are dynamically reorganized between the first postnatal day and day 28…. The sensory experience (light) plays a major role in sculpting the zinc-containing innervation of the visual cortex.”
It is at this time in the early development of a child that ocular dominance is determined. Stripes of brain cells called ocular dominance columns in the visual cortex of the brain in some mammals and humans preferentially respond to input from light.
The theory that zinc deficiency induces dyslexia was confirmed in 1988 when researchers measured sweat and
urine of dyslexics among paired children (one normal child paired with a dyslexic child) and in 25 of 26 paired children the dyslexic child had lower zinc levels.
Researchers wrote: This study shows clear evidence of an association between dyslexia and low concentrations of zinc in sweat. Dyslexic children also tended to have higher copper levels. Zinc and copper balance each other.
In animals zinc deficiency during pregnancy can cause learning impairment, behaviour disorders, and immune dysfunction persisting for several generations.
In 1988 researchers said prospective studies of zinc and the effects of supplementation before conception, during pregnancy, and in early childhood “are urgently needed.” That was over 25 years ago.
Dyslexia still continues unabated. No preventive measures are in play. The zinc-link goes unrecognized. Inform parents of dyslexic children about this and they seem bewildered. With no other sources to reference, they may ask their doctors, who know nothing about this. Some mothers, hearing about zinc, begin to wonder now if it was something they did wrong to bring about the dyslexia in their child. They wonder if they should blame themselves.
Bring the prospect of zinc supplementation being a remedy for dyslexia to the attention of a teacher who specializes in tutoring dyslexic kids to read and the teacher may have mixed emotions. They won’t be needed as much if kids find a way out of their dyslexia. While dyslexic kids need zinc, dyslexia will still be a challenge throughout life.
A white moon at the base of the nail bed is a sign of zinc deficiency. I have a dyslexic child with dissipating white nail beds as he supplements his diet with zinc. I have yet to examine the nail bed of a dyslexic child who does not have that sign.
Oddly, while zinc is an essential nutrient that is in short supply in the diet, parents often guardedly consider the idea of zinc supplementation for their child, feeling they do not have enough information to make such a decision on their own. But parents inexplicably place their kids with behavioral issues on stimulant drugs like Ritalin without hesitation.
What harm could come from zinc supplementation? Most children are picky eaters and without zinc supplementation are prone to infections, the most common being chronic ear infections that can lead to hearing loss, often from the toxic effects of antibiotics.
Without zinc children do not make sufficient memory antibodies that provide them with lifetime immunity. Without zinc vaccines don’t work well.
Young infants are commonly seen in pediatricians’ offices with overt signs of zinc deficiency, such as recurrent infections, irritability, diarrhea, skin rash, other skin problems, failure to grow, poor appetite, particularly infants born preterm, yet it never crosses the mind of the doctor the infant is zinc deficient.
As the child grows he/she may show other signs of zinc deficiency (and copper overload) such as salt craving, skin problems, sweaty feet (smelly socks), constipation, poor wound healing, failure to grow (short stature), allergies, alopecia (hair loss).
A vegetarian mother who is pregnant would be putting her newborn at risk for zinc deficiency just when it is needed after birth for mental and visual development. Zinc therapy is documented but an overlooked therapy for hyperactive children.
Dyslexia is not the only visual problem that emanates from a shortage of zinc. Zinc is needed for proper vitamin A utilization. Vitamin A converts to a visual chemical (rhodopsin) that may be in short supply and result in impaired night vision. Zinc is required for rhodopsin.
To make matters worse, inadequate zinc intake may often result in infants and children being fussy eaters with poor appetite, which further reduces zinc intake.
In adults up to 40 milligrams is completely safe. Due to growth, children have higher demand for zinc than adults. However, excessive zinc supplementation may be counterproductive as more zinc is bound up to a molecule called metallothionein. However, this binding prevents toxic effects of overdose.
Zinc oxide is poorly soluble in water, the most economical zinc supplement sold in health shops, is poorly absorbed. More absorbable forms of supplemental zinc are zinc acetate, gluconate, methionine, citrate. The co-consumption of vitamin B6 with zinc increases absorption and selenium releases zinc so it can be utilized.
Many young children are zinc deficient. Outside of oysters, there are no zinc-rich foods. Maybe 10% of dietary zinc is absorbed. Typical adult intake of zinc from the diet is ~10 mg per day, but outside of fortified cereals (Cheerios 16 mg) and beverages (Ovaltine 3 mg), young children simply do not commonly consume foods said to be rich in zinc. Kids may consume 1-2 mg of zinc per day and less than that is absorbed.
Mothers who take a report like this to their children’s doctor are often dealt with by ordering a zinc blood test to appease the parents. However, zinc blood levels only reflect recent consumption and are notoriously inaccurate because zinc is often un-utilizable when bound to metallothionein.
Also a child’s blood zinc level is compared against the so-called “reference range,” that is what is normally occurs among subjects undergoing blood tests at that laboratory. So if there is mass deficiency (as there is with zinc), then the reference range is what normally occurs but is then, by deduction, the child is normally (commonly) deficient along with everybody else!
Blood plasma levels of zinc do not correlate with zinc intake. Patricia Hausman in her book THE RIGHT DOSE explains: “the best proof of zinc deficiency is the presence of some of its typical symptoms followed by improvement or disappearance after supplementation.” However, remember if zinc supplementation doesn’t resolve symptoms it may be due to a lack of absorption or release from its binding protein.
Posted in Brain, Dietary Supplements ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105