
Sign up for periodic reports and bulletins

Bill Sardi
the vitamin supplement answer man
FREE access; FREE of commercials; FREE to use
Sign up for periodic reports and bulletins
FREE access; FREE of commercials; FREE to use
Posted April 29, 2020: by Bill Sardi
While laboratories around the world are racing to develop a safe and effective vaccine against the mutated coronavirus, now known as 2019-nCoR, which is said to have killed hundreds, and with rumors Chinese health authorities are hiding more dead bodies underneath the floor boards of their newly constructed coronavirus hospitals, there is already a non-vaccine cure.
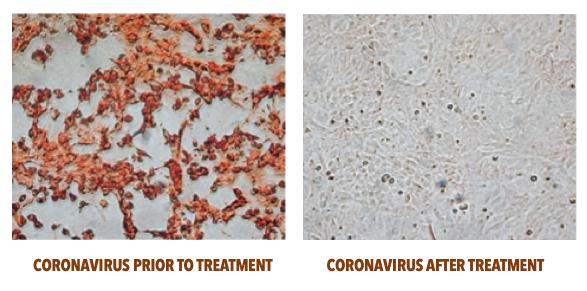
Convincing visual lab-dish evidence is shown below. (Because bots read these reports and censor them or bury them on obscure web pages when they refer to natural remedies, you need to click here for the identity of the cure. Otherwise an online search would have been unlikely to find this this report.)
Certainly, don’t tell a new world order organization called the Coalition for Epidemic Preparedness Innovations (CEPI) about this coronavirus cure. CEPI is handing out research grants to develop a vaccine. This is free money to pharmaceutical and biotech companies and actually the whole reason for the conjured up epidemic, to develop a vaccine with public money.
CEPI is a private/public coalition headquartered in Norway with $760-billion of funding by various countries, the Wellcome trust and the Bill & Melinda Gates Foundation.
Recognize the billion-dollar reward a pharma/biotech company could gain from approval of such a vaccine. Why, it would make a pre-planned “killing” in the stock market, as three such companies have been awarded research grants by CEPI.
CEPI is not just a funding agency. As Science Magazine report says: “CEPI supports began within hours after Chinese researchers first posted a sequence of 2019-nCoR in a public database. That happened on Friday evening, 10 January, in Bethesda, Maryland, home of the U.S. National Institute of Allergy and Infectious Diseases (NIAID).”
CEPI researchers began to analyze the sequence of genes within the virus the next morning. The genetic makeup of the WUHAN 2019-nCoR is said to be 80% similar to the SARS virus (Severe Acute Respiratory Syndrome) that erupted in 2003 that reportedly killed 774 worldwide.
What has part of the world on lockdown is the news-media-generated fear of this rarely mortal, slow-to-spread virus. In an overkill by the World Health Organization, when air travelers return home from a trip to China they are placed in quarantine for two weeks.
The current fear being spread over the 2019-nCoR viral epidemic appears to be a drill to test public health quarantine measures. As onerous as these quarantines are, it appears these extreme measures have been no more effective in preventing deaths in 2019-2020 compared to the SARS epidemic of 2003.
As of February 8, 34,958 cases of coronavirus have been confirmed and 724 deaths worldwide (2% died). According to the Centers for Disease Control, the 2003 SARS outbreak reportedly infected 8,098 people and resulted in 774 deaths (9.6% died).
As of February 7 there were 24,953 cases in Wuhan and its environs, a city of 11 million. Presuming all cases of coronavirus in greater Wuhan have been reported to health authorities, the risk for infection would only be 6 in 100,000, a very remote risk. The risk for death is even more improbable. Yet everyone will be expected to be inoculated once a vaccine is developed, approved and available.
In other words, if a vaccine were developed for this 2019-nCor coronavirus, 16,666 people would need to be vaccinated to prevent 1 case of coronavirus infection. So, off the top, given the high number of people needed to vaccinate to prevent just one case of viral illness, vaccines would be categorically ineffective and costly.
If a vaccine were developed for this 2019-nCor coronavirus, 16,666 people would need to be vaccinated to prevent 1 case of coronavirus infection.
Let’s assume that all coronavirus infections have been reported to health authorities in Wuhan, China.
Let’s assume the occurrence of severe side effects from any upcoming approved 2019-nCoR coronavirus vaccine were the same as flu shots.
Let’s presume 15% of Wuhan’s population is over age 65 and a vaccination rate of 100%. That would amount to 1,650,000 vaccinated elderly individuals.
Let’s use a study of senior adults in the U.S. (a well-fed population) that received standard and high-dose inactivated trivalent (three strains) flu vaccine for comparison, where severe side effects were reported for 0.6% and 1.3% of vaccinated subjects respectively.
Given that the infection rate in a population such as Wuhan is just 1 in 16,666 without vaccination in the population overall, and a higher anticipated rate of infection would be expected among senior adults, let’s say 30%, which would amount to 4,999 infected among every 16,666 elderly Wuhan residents. That would amount to 495,000 coronavirus infections among an estimated 1,650,000 elderly unvaccinated residents of Wuhan.
Let’s presume any newly approved coronavirus vaccine is only 50% effective at reducing coronavirus infections rates among elderly Wuhan residents based upon recent data for vaccine effectiveness studies for flu vaccine. So maybe 247,500 cases would be prevented out of an estimated population of infected and uninfected population of 1,650,000.
If the current death rate from coronavirus of 2% among infected individuals is factored, then an estimated 4950 lives out of 247,500 infected patients would be spared due to vaccination.
Using the data from a U.S. population of similar age (cited above), severe side effects would be expected to occur in 216-1000 of every 16,666 vaccinated senior adults. Therefore, an estimated 21,384-99,000 out of 1,650,000 vaccinated senior adults in Wuhan would be expected to experience severe side effects from the vaccine leading to hospitalization. How many vaccine-related and treatment-related deaths would occur is unknown. Severe side effects and possibly vaccine/treatment-related deaths would vastly outnumber the number of lives saved via vaccination.
|
CORONAVIRUS PROJECTED NUMBERS IN WUHAN, CHINA |
|
| Coronavirus infection rate in Wuhan, China, current |
1 in 16,666 |
| Estimated population of elderly in Wuhan (15% of 11 million)- presume 100% are vaccinated |
1,650,000 |
| Coronavirus infected elderly in Wuhan (estimated)- 30% |
495,000 |
| Infections prevented, 50% effectiveness of coronavirus vaccine |
247,500 |
| Estimated lives saved due to vaccination; presume vaccine prevents all deaths among 247,500 elderly; 2% death rate |
4,950 |
| Predicted vaccine-induced severe side effects among elderly Wuhan residents (all are hospitalized) |
21,384-99,000 |
| Vaccine-related/ treatment-related deaths
1/10th of 1% vaccine/treatment-induced deaths would = 1650 deaths |
?? |
Those widely publicized instant-built hospitals in Wuhan for the coronavirus would largely be filled with patients suffering severe vaccine-related side effects, not the coronavirus infection itself.
My comparisons herein are more than fair to an imagined coronavirus vaccine because I’m comparing vaccine effectiveness and side effect data from healthy elderly U.S. populations versus actual data from the current coronavirus in a presumably less healthy older population suffering from a coronavirus epidemic now underway in Wuhan, China.
Once mass vaccination would be forced upon the population in China, hospitals would fill with patients experiencing severe vaccine-induced side effects and would be easily confused with cases of severe coronavirus infection, leading to needless public panic, fear and needless death from treatment-related causes. Iatrogenic (treatment-induced) deaths would further worsen outcomes.
Serious side effects from flu vaccination include:
Note: It is difficult to locate a list of severe side effects caused by flu vaccination. There is online censoring of information about serious side effects of vaccines. An online search conducted for “severe side effects, flu vaccine” redirects and never leads to a source that lists severe side effects. Try this search for yourself.
Given that coronavirus vaccine would likely be in limited supply a CEPI representative says: “It appears at this point in time that older individuals, probably immune-compromised individuals, individuals with other medical conditions seem to be the ones who are affected the most by the severe disease… Each country needs to prioritize whatever vaccine becomes available for those who are identified as being at the highest risk.”
Finally, an admission that there are only a small number of people who are at high-risk to develop coronaviral infections and, by the way, they happen to be the least likely to successfully develop antibodies to any virus following vaccination.
Why would the elderly be most vulnerable to coronavirus?
Answer: Because they don’t develop adequate antibodies.
So, the moronic response is either to develop a vaccine that contains an attenuated version of the virus itself and hope and pray it works in an immune compromised elderly adult population, or maybe even inject antibodies directly into at-risk individuals.
A report published in the Proceedings of the National Academy of Sciences notes the development of an antibody that binds to a coronavirus that would serve as prophylaxis against infection.
(Need coronavirus antibodies? You can purchase coronavirus antibodies online -$358 for a quarter of a milligram. But you just have to be a certified research lab to order.)
One plan is to develop antibodies that bind to viral proteins and, in doing so, stop the pathogen from readily infecting human cells. Some scientific excitement surrounds the development of compound CR3022 which is said to bind and combine with antibodies that attack coronaviruses.
But why the search for antibodies against coronavirus when your body already has an organ dedicated to making them—the thymus gland (located under your breast plate)?
With potentially seven strains of coronavirus in play, researchers are searching for a broad-spectrum remedy. But RNA viruses like coronavirus have high mutation rates – up to a million times greater than their host cells. So just how can a vaccine be made that specifically protects against a strain of coronavirus when the virus itself is mutating mid-season?
Of interest, in the search for a broad-spectrum coronavirus treatment, zinc-based drugs were explored.
That is no surprise, given that zinc deficiency is associated with increased susceptibility to infectious diseases caused by bacterial, viral, and fungal pathogens. The particular type of immune cells that are affected by zinc deficiency are T lymphocytes. The T stands for thymus gland. These glandular T-cells are reduced in number by zinc deficiency. A shortage of zinc also reduces the secretions (thymulin) from the thymus gland.
When viral particles enter the blood circulation they are confronted by so-called naïve T-cells that have not made any antibodies yet. These T-cells aren’t very active without zinc. In fact, the thymus gland itself shrinks from the size of a walnut in adulthood to that of a pea without adequate zinc. Antibody responses are reliant upon zinc.
One report concedes zinc supplementation could improve vaccination success rates. This is the primary reason why vaccines are ineffective, particularly among the very young (under age 2) and the very old (over age 65) who typically have low blood levels of zinc. High zinc deficiency rates are reported in China (50-70% in children and 31% in adults)
Instead, toxic adjuvants like mercury and aluminum are inhumanely added to vaccines to provoke an antibody immune response. But zinc therapy is ignored by modern medicine.
International Journal of Antimicrobial Agents
Available online 24 April 2020, 105995
https://www.google.com/search?q=interferon&oq=interferon&aqs=chrome..69i57j0l7.2503j0j8&sourceid=chrome&ie=UTF-8
Coronavirus disease 2019 (COVID-19) caused by a previously unknown pathogen named severe acute respiratory syndrome-related coronavirus-2 (SARS-CoV-2) has now become a pandemic threat to the whole world. However, there are no vaccines or specific treatment against the new virus. Therefore, there is an urgent need for advancing novel therapeutic interventions for COVID-19. Glycyrrhizin, a triterpene saponine from licorice root, is valuable for its various biological functions and pharmacology effects. In this brief article, we will discuss the therapeutic potential of glycyrrhizin for COVID-19 coronavirus infections from the perspective of its pharmacological action including binding angiotensin converting enzyme II (ACE2), down-regulating pro-inflammatory cytokines, inhibiting the accumulation of intracellular reactive oxygen species (ROS), inhibiting thrombin (blood clots), inhibiting the hyperproduction of airway exudates, and inducing endogenous interferon(anti-viral defense).
Posted in Coronavirus ; No Comments »
11
17
52
95
14
24
237
6
56
43
10
116
15
66
105